Download
1 / 52
690 likes | 1.67k Views
PHYSIOLOGY OF SLEEP & BREATHING. John KOLBE Respiratory Services Green Lane Hospital, & Faculty of Health Science University of Auckland. .

E N D
PHYSIOLOGY OF SLEEP & BREATHING. John KOLBE Respiratory Services Green Lane Hospital, & Faculty of Health Science University of Auckland.
To die, to sleep; To sleep: perchance to dream: ay, there’s the rub; For in that sleep of death what dreams may come When we have shuffled off this mortal coil, Must give us pause. William Shakespeare “Hamlet”.
What hath night to do with sleep? John Milton “Comus”: 1637.
SLEEP (Oxford) “Bodily function such as that which normally recurs for several hours per night in which the nervous system is inactive, eyes closed, postural muscles relaxed and consciousness nearly suspended.”
SLEEP (Scientific) Sustained quiescence in a species, specific state accompanied by reduced responsiveness to external stimuli. Additionally in mammals; - quick reversibility to the wakeful condition - characteristic EEG changes - ?spontaneous occurrence with endogenous periodicity
WHY DO WE SLEEP? So we ain’t knackered, guv?
Function of Sleep. • ? • Mammals and birds have similar sleep physiology • Brain Metabolic Restoration • Remodelling of synaptic function • Energy Conservation • Reduction by only 10% • Enforced Immobility
Sleep-Wake Cycle. • Push-Pull system • Circadian clock in suprachiasmic nucleus • Sleep drive/promotion- solitary tract nucleus, raphe nucleus,medial forebrain area • Related to duration of wakefulness and duration & quality of last sleep • Inhibition of reticular-activating system- alertness/wakefulness promotion: • Chemical influences • IL 1, TNFa, serotonin, adenosine (inhibits caffiene) promote sleep; PGE2 inhibits sleep
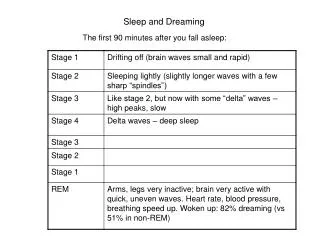
STAGES OF SLEEP Deeper Sleep 5 Stages Non-REM Sleep - Stage 1 - Stage 2 - Stage 3 } Slow Wave Sleep - Stage 4 } REM Sleep (motor activity is inhibited)
Stages of Sleep. • Awake alpha rhythm • Non-REM • 1 alpha to theta • 2 sleep spindles,K complexes • 3 • 4 SWS – thalamocortical burst activity ( delta waves) Fall in ventilation, CO, heart rate, blood pressure.
SLEEP PHYSIOLOGY REM and non-REM sleep alternate cyclically REM sleep: - 20-30min every 90-120 min - increases later in night
Stages of Sleep. • REM • Interaction between cholinergic activation and monoaminergic inhibition • cerebral metabolic activity • CNS excitation (dreaming) • Intermittent eye movements • inhibition of motor activity, loss of postural tone • Autonomic variability,cardio-respiratory instability
SLEEP IN NEWBORN & INFANTS Enter sleep through REM (active sleep) NREM-REM cycle, 50-60 min from birth REM may be up to 50% of total ECG patterns on non-REM emerge between 2-6 months and consolidate into sleep cycle SWS becomes prominent when brain structure and function develop.
SLEEP IN CHILDREN. • SWS dominates • Awakening children in first SWS cycle may be difficult • Amount of SWS decreases progressively thru’ the second decade to account for 15-52% of sleep at end of teens.
Sleep Architecture in Young Adults Sleep is entered through non-REM NREM and REM sleep alternate within period of 90-120 mins SWS predominate in the first third of the night and linked to sleep initiation - approx 20 % of total REM sleep predominates in the last third of the night and is linked to circadian temperature rhythms - 20-25% of total.
SLEEP ARCHITECTURE IN YOUNG ADULTS Wakefulness in sleep, <5% of night Stage I 2 - 5% Stage II 45 - 55% Stage III 3 - 8% Stage IV 10 - 15% NREM 75 - 80% REM 20 - 25% in 4-6 episodes
Effect of Age on Sleep SWS fades with age (halves cf adolescents) By 60 years no SWS in some men (loss of cortical synaptic density) REM % of sleep is maintained in health old age (?relates to intellectual functioning) Arousals increase with age Marked variation
STRUCTURE OF HUMAN SLEEP Amount favoured by an individual is highly variable (4-10 hours) Amount needed is unclear, performance falls off <5-5.5 hours for most Sleep deprivation leads to a “sleep debt” of SWS and REM Proportions of each stage vary with age - significance unclear
Required Duration of Sleep. • Highly variable • 6.5-8.5 hrs • Sleep deprivation; major impact on • Cognition • Speed of performance
Sleep Deprivation. • Acute • Rebound increase in SWS • Followed by rebound increase in REM • Chronic • Disturbance of the usual sleep stage pattern during catch-up; bizarre phenomena like “sleep onset” REM.
Sleep Deprivation = Disaster. • Chernobyl • Exxon Valdiz • Three Mile Island • Challenger Space Shuttle.
Structure of Human Sleep Cont. Sleep patterns are very much habit and humans can adapt to bizarre sleep patterns and appear to function effectively Shift workers have increased physical and psychological morbidity Lack of SWS postulated to lead to loss of psychomotor performance Lack of REM postulated to lead to irritability, mood swings etc.
NON-REM SLEEP & BREATHING Respiratory drive - stim effect of wakefulness - chemosensitivity Fluctuations in respiratory drive (in stage 1&2) Non-chemical respiratory inputs are minimised. Breathing regulated by metabolic respiratory control (in deeper stages, stable) VE and slight PaCO2
REM SLEEP & BREATHING Irregular respiratory drive Ventilatory response to chemical and mechanical stimuli may be transiently reduced or abolished Short periods of (central) apnoea occur Intercostal and accessory muscle activity Generalised inhibition of skeletal muscle tone (including pharyngeal muscles) Thoraco-abdominal coupling
BREATHING DURING SLEEP • Clinical significance • Control of breathing • Sleep Physiology • Breathing during sleep • Patho-physiology of breathing during sleep
PHYSIOLOGIC IMPACT OF SLEEP ON BREATHING • Very little in normals • Very important consequences in those with disturbances of respiratory structure or function eg - metabolic drive - diaphragmatic strength - intercostal and accessory muscle function activity ( imp in those with structurally small oropharynx)
Pharyngeal Musculature • principally pharyngeal dilators/stabilisers - genioglossus is predominantly an inspiratory phasic muscle - tensor palatonic is a tonic postural muscle • are “respiratory” muscles (output from CNS) • respond to standard respiratory stimuli viz CO2, O2 • respond to negative pressure via superior laryngeal nerve
Sleep and Pharyngeal Muscle • Inspiratory phasic muscles eg genioglossus, have near normal activity during sleep • Tonic postural muscles (tensor palatini) activity • Upper airway resistance increases during sleep in normals (x = 3) as a result of tonic muscle relaxation snoring
Snoring •Risk factors include males gender, obesity, alcohol /sedatives •Not necessarily benign; associated with - CAD risk - Hypertension - cerebrovascular risk •In isolation is a poor marker for OSA (<50% of snorers suspected of OSA have AHI >10) Not indication in itself to progress to sleep study unless other features present (eg witnessed apnoeas, hypersomnolence)
Great eaters and great sleepers are incapable of doing anything that is great. William Shakespeare “Henry IV”
OSA Pathophysiology • UAW obstruction at level of tongue/palate • Size of UAW lumen is a balance between - tendency of pharynx to collapse during inspiration - dilating forces (pharyngeal muscles)
Mechanisms of Obstruction. Airway Dilating Muscles. Obesity Retrognathia Sleep Alcohol Age Pharynx
Sleep Problems. • Common • 10% have insomnia • 10-20% of partners annoyed by snoring • 2% of adults have a medical cause for pathological sleepiness • 1-4% of older males have OSAHS
Sleep History. • I Insufficient sleep and insomnia • S Snoring and shift work • N Narcolepsy/cataplexy • O Obstructive apnea • R Refreshing sleep • E Excessive daytime sleepiness • D Drugs – sedatives & stimulants.
Sleep Hygiene. • Don’t have a fixed bedtime • Do have a fixed get up time • Do limit your activities in bed • Don’t stay in bed if fully awake • Don’t nap during the day • Do exercise
Sleep Hygiene. • Do have a bedtime ritual • Do banish clocks • Don’t use bed as a place to solve problems • Don’t worry if you do not sleep.