Download
1 / 23
230 likes | 242 Views
This presentation discusses the underreporting of melanoma cases and explores the reasons behind it. It also suggests actionable solutions to improve reporting accuracy and identify high-risk population subgroups.

E N D
Melanoma underreporting:how big is the problem andhow do we fix it? June 16, 2009 NAACCR 2009 Annual Conference San Diego, California Christina Clarke, Ph.D Susan Swetter, MD David Peng, MD Theresa Keegan, Ph.D Dennis Deapen, Ph.D Myles Cockburn, Ph.D
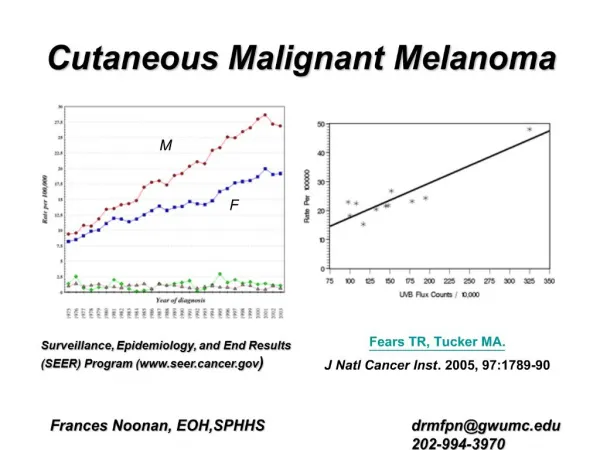
The burden of melanoma is increasing… • Cancers of melanocytes with particular propensity for metastasis • Therefore, early detection of utmost importance • Incidence rates increasing 3-4% per year • among the most rapidly increasing cancers in US whites • Quantifying burden critical for • Evaluating primary prevention and screening programs • Targeting population subgroups for primary and secondary prevention
…but are adequate resources being marshalled? • Are current quantifications of melanoma occurrence accurate? • Capturing rate of increasing trend? • Defining population subgroups at greatest risk? • Several prior efforts have pointed to nonreporting and delayed reporting of melanoma
Objectives of presentation • Describe reasons for under- and nonreporting of melanomas • Describe efforts to understand extent of underreporting in California • Suggest some actionable solutions
Melanomas differ from other cancers Diagnosis tipped off by visual examination + Treatment relies mainly on surgery + Adoption of narrower excision margins + Use of Mohs micrographic surgery for superficial melanoma + Otherwise increased diagnosis and treatment in physician offices or outpatient settings = Increasing numbers of thin melanomas being diagnosed, reviewed and treated outside of existing hospital-based cancer reporting systems
How are new melanoma cases being identified now? In Los Angeles…. • 50% from hospitals • 30% from pathology labs • 1% by physicians using confidential morbidity report (CMR) cards • 19% from active follow-back of pathology records reporting “clear margins” Inside established reporting system
How melanomas get missed • Large proportion of cases requiring active casefinding by cancer registry • Must know about and establish relationships with new or out-of-state pathology laboratories • Must have records or e-path to follow-back all clear margin reports • Must know about and solicit reports from community physicians diagnosing melanomas • Registry does not have resources to do all these
SEER Rapid Response Special Studies • Aims • Identify and interview full census of regional dermatologists and physicians diagnosing melanoma to • ask about reporting practices • ask about pathology resources being used • ask how many melanomas are being diagnosed • identify previously unknown pathology laboratories • Estimate impact of missing cases • Coordinated efforts by two California SEER regions • Los Angeles (2005-2006) • Greater Bay Area (2006) • Collaborations with local dermatologists • Drs. Susan Swetter (Stanford) , David Peng (USC)
Survey methods • Create regional census of dermatologists and dermatopathologists • Obtain comprehensive member listings for region • AMA (Dermatology; Dermatopathology • American Academy of Dermatology (local division) • American Association of Dermatologic Surgeons • American Society of Dermatopathology (local) • American College of Mohs Micrographic Surgery • Internet searches for “dermatologists” and “dermatopathologists” working in region • Obtain from cancer registry names of any physicians reporting melanomas in past 5 years • Carefully check for updated address or telephone numbers • Interview dermatologists or their office managers • Los Angeles: telephone only • Greater Bay Area: first offered self-administered paper, fax, or internet version, then telephoned non-responders • Confirm eligibility • Not retired or relocated in past year; still practicing dermatology
Numbers of dermatologists contacted • Los Angeles (2005-2006) • 701 identified • 145 determined ineligible • 235 could not be reached or did not respond • Of 556 eligible, 321 interviewed (58% response rate) • Greater Bay Area (2006) • 495 identified • 26 could not determine phone number or address • 85 determined ineligible • 10 declined to participate • Of 410 eligible, interviewed 339 (83% response rate)
Key findings: more melanomas diagnosed than reported • Los Angeles (2005-2006) • Respondents estimates of numbers diagnosed 30-40% higher than those actually reported in registry • Greater Bay Area (2006) • Respondents estimates of numbers diagnosed 38% than those actually reported in registry • After excluding several impossibly high estimates of >1000/cases/5 years • Estimates probably high due to non-consolidation but also exclude survey non-responders who are also most likely to be melanoma non-reporters
Key findings: pathology laboratories see most cases • Over 80% of respondents indicated that they did not review their own slides and used an outside lab • Los Angeles (2005-2006) • Respondents listed 21 laboratories not known to registry • Greater Bay Area (2006) • Respondents listed 6 out of-state laboratories not known to registry • 27 (7%) dermatologists reported performing Mohs micrographic surgery • Changing outpatient diagnostic/surgery practices not a major source of missing cases
Key findings: very few physicians report directly to registry • Los Angeles (2005-2006) • 3% of physicians reported using CMR cards • Many reported that they ‘waited for a follow-up from registry” • Most physicians who said they did not report directly to registry asked “Why, am I supposed to?” • Greater Bay Area (2006) • 95% said they assumed all reporting was being taken care of by their hospital or pathology service • A great deal of confusion exists as to cancer reporting obligations, regulations, and procedures • Assumptions that it is “someone else’s job”
Options for concerned registries • Conduct regular audits of all pathology laboratories • $$$, labs are increasingly out of state • Make sure all pathology services are reporting referral cases • One large dermatopathology service in Greater Bay Area was not reporting referrals, thought they were “someone else’s job” • Change current follow-up processes to target the few facilities that appear to be worst offenders • Mission critical: convince large numbers of physicians to report their (small numbers of) melanomas
Educating physicians about melanoma reporting • Dermatologists clearly want melanomas to be reported but might not know • Their legal obligation to do so • How to do it • First, make it as easy as possible for them to report • Offer secure web-based systems for physician reporting
Educating physicians about melanoma reporting • Registries should be proactive in reaching out to local dermatology communities • Registries at universities can engage with institutional colleagues • Offer to make a presentation at local derm society meeting • Emphasize that under-representing the extent of the melanoma epidemic shortchanges funding for melanoma research and screening • Disseminate the “melanoma reporting checklist” • Send them a copy of JAAD article • PDF available by request! • Posted online at www.countallmelanomas.org