Download

1 / 19
190 likes | 200 Views
Parent Training for teatimes without tantrums. Evidence Based Practice, Feeding Disability. Presentation overview. Orientation videos The paediatric feeding caseload of community speech pathologists. Development of clinical question

E N D
Parent Training for teatimes without tantrums Evidence Based Practice, Feeding Disability
Presentation overview • Orientation videos • The paediatric feeding caseload of community speech pathologists. • Development of clinical question • Qualitative literature- parents and professional perspectives of feeding intervention and management. • Critically appraised papers • Clinical conclusions and applications • Clinical practice of feeding speechies • Where to from here.
Peadiatric feeding (disability caseload) Who? Children with a range of feeding difficulties. From birth through to adulthood.
Development of clinical question • Interest in best utilising the time we have with parents to help them develop confidence and skills to manage their children’s feeding difficulties. • Is parent training effective? Will it improve feeding outcomes? What type of parent training?
Clinical question For children with feeding difficulties does parent (or carer) training improve feeding outcomes? • Can parent training be an isolated intervention strategy? • Which methods? • How? • For how long? • For which types of client?
Placing the evidence within our clinical practice. • Survey distributed to 30 ADHC speech pathologists from across Sydney metro. • Qualitative information to allow comparisons to findings in the literature with everyday clinical practice. • A range of clinical caseloads and therapist experience in survey results. • Identifying what SPs feel works and doesn’t works in terms of
What strategies do we already use to train parents around mealtime skills?
Search results • Search terms • Where we looked • What we found • CAP for 4 articles (to follow)
What does qualitative research tell us about the effectiveness of dysphagia/feeding intervention? • Behavioural modification training is cited widely in the psychology literature. For example, Training included teaching reinforcement and prompting strategies for 10 kill components through using verbal explanations, demonstrations of appropriate and inappropriate responses and role plays the children's' fast-food restaurant skills improves and were maintained for 4 mths and training program influenced the parents' teaching interactions with their children
ARTICLE 1Turner, K.M.T., Sanders, M.R., & Wall, C.R. (1994). Behavioural parent training versus dietary education in the treatment of children with persistent feeding difficulties. Behaviour Change, 11(4), 242-258. Method Randomised group-comparison design. 2 treatment conditions (Behaviour Parent Training and Standard Dietary Education). Results Behavioural Parent Training is more effective at increasing positive mother-child interactions than Dietary Education and leads to increased parental satisfaction with treatment. However, there is no significant difference between the interventions at improving children’s mealtime behaviours, their dietary intake or anthropometric measures.
ARTICLE 2 Aim To determine if using preferred foods motivates children in consuming less preferred foods and, in turn, improve food refusal. Method -parents taught to teach a consistent procedure when presenting the new foods He was told he would have to eat a small amount of the new food before he could have his preferred food Verbal praise was used Results -The subject immediately ate small quantities of the new food that he was presented with. He then accepted increased quantities of the first two foods and new flavours with the third. At 3 mth follow up, he was continuing to eat increasing amounts of the presented foods.
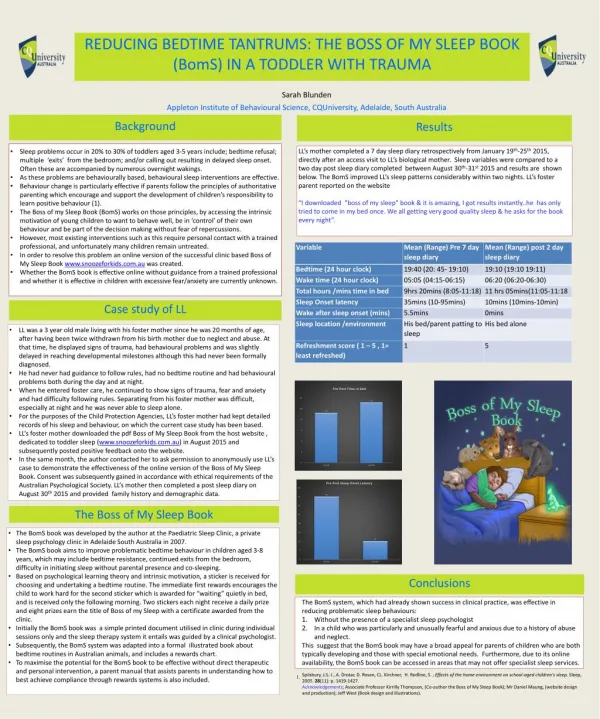
ARTICLE 3Stark L J et al (1994). Modifying Problematic Mealtime Interactions of Children with Cystic Fibrosis and their Parents via Behavioural Parent Training. Method Pre and Post measures. Baseline measures – weight - calorie intake - Global Rating Scale for Feeding Situations (GRSFS). Parents kept weight and food diaries. Sessions were provided once/week for 90mins, with twice weekly video-taped home meals. Review of vignettes from families, vivo practice in behaviour management techniques. Parents were instructed to provide verbal praise of appropriate child eating behaviours and to ignore complaints about foods, inappropriate behaviours and food refusal. Follow up sessions at 3 and 8 months post treatment for younger child’s family and 1 and 12 months post treatment for older child’s family.
Cont…ARTICLE 3Stark L J et al (1994). Modifying Problematic Mealtime Interactions of Children with Cystic Fibrosis and their Parents via Behavioural Parent Training. Results Child one: Appropriate eating behaviours immediately improved an disruptive behaviours reduced. Over time behaviours varied but always stayed rated as “high”. Caloric intake increased and was maintained. His weight percentile improved from 55 to 93 at the review. Child two: Appropriate eating behaviours also immediately improved but over time had decreased to moderate and at follow up was rated again as high. Disruptive behaviours reduced and over time had increased, but at follow up was rated as low. Caloric intake initially increased for one client, followed by a small increase at first follow up, then small decrease at second follow up. Caloric intake slightly decreased (bottle reduced, and solid intake increased). Weight percentile slightly decreased from 90 to 88.
Stark L J et al (1994).Modifying Problematic Mealtime Interactions of Children with Cystic Fibrosis and their Parents via Behavioural Parent Training. Method Results
In 2011… Meetings will take place at Rosebery ADHC office. Level 3, 61 Dunning Avenue, Rosebery 2018 Please contact Emma Chapple emma.chapple@dhs.nsw.gov.au phone: 9310-6300
Next year for paed feeding (disability) • Fussy eaters • Dysphagia and schools • Group therapy for problem feeders
Laura Mobbs (ADHC, Hornsby) • Tsen Levsen (ADHC, Rosebery) • Jo Scaltrito (Kogarah D&A) • Rachel Cummins (ADHC, Campbelltown) • Kylie Ryan (ADHC, Campbelltown) • Carmen Newton (ADHC, Hurstville)
References • Stark L J et al (1994).Modifying Problematic Mealtime Interactions of Children with Cystic Fibrosis and their Parents via Behavioural Parent Training. • Turner, K.M.T., Sanders, M.R., & Wall, C.R. (1994). Behavioural parent training versus dietary education in the treatment of children with persistent feeding difficulties. Behaviour Change, 11(4), 242-258.