Download
1 / 10
110 likes | 256 Views
NSCLC. Preoperative CT. Resectable disease Stage III Patients. Stage IIIA Preoperative CT Less competition but opportunity to take: NAVELBINE GEMZAR TAXOL TAXOTERE. NSCLC Main drugs. 91% (N 1 ) 87% (N 2 ). 78% (N 0 ) 76% (N 1 ). 100. 90. 66%. 62%. 80. 70. 39%. 60. 50.

E N D
NSCLC Preoperative CT Resectable disease Stage III Patients
Stage IIIA Preoperative CTLess competition but opportunity to take: NAVELBINE GEMZAR TAXOL TAXOTERE NSCLCMain drugs
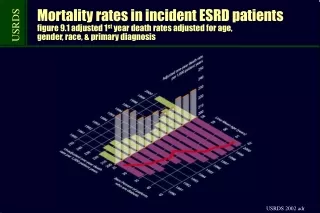
91% (N1) 87% (N2 ) 78% (N0) 76% (N1) 100 90 66% 62% 80 70 39% 60 50 40 30 20 IA IB IIA IIB IIIA 10 0 Early stageNSCLC 5-year mortality rate from time to surgery Local relapse 30% 21% 10% Distant relapse70% 79% 90% Distant recurrence remains the major cause of treatment failure Mountain,Chest 97
Early stageNSCLC How to reduce the risk of distant recurrence ? • Adjuvant treatment: Awaiting results of international trials (ANITA, IALT, NCI, BLT, ALPI) • Neoadjuvant treatment: Preoperative CT improves survival in IIIA patients and even earlier stages who can be completely resected Roth J. Lung Cancer 98; Rosell R. Lung Cancer 99; Depierre A. JCO 02; André F. JCO 00
Navelbine + CDDP NAVELBINE 30 mg/m² D1, D8 CISPLATIN 80 mg/m²D1 every 3 weeks Spasova Phase II study n= 56 stage III pts OR54%Significantly longer survival pCR3 ptsfor responders (21 m. vs 9 m. p< 0.001) Complete32%Significantly longer survival for resectioncompletely resected patients (28 m. vs 11.5 m. p< 0.001) 1-YS59% 2-YS27% NAVELBINE allows survival improvement Spasova I et al. Eur. J. Cancer Vol 37 01
Navelbine Experience2-3 drug combination with CDDP 9 studies, n= 257 pts Stage IIIA-B EFFICACY OR : 54-78% Resection : 43*-80% Complete Resection : 32-55% 1YS : 65-70% 2YS : 41% TOXICITIES NP Leucopenia G3 : 16% cy. Anemia G3 : 13% cy. NIP Feb. Neutropenia : 13% pts Alopecia G3 : 84% pts N/V G3 : 3% pts *all patients = IIIB
A new approach with Navelbine:CT-RT preoperativetreatmentPhase II trial NVB 17.5 mg/m²/week CBDCA AUC 6 D1 RT 45 Gy Garst study n= 30 (stage IIIA) EFFICACY OR: 70% pCR: 10% Resection : 87% 1YS : 80% 2YS : 53% Garst, ASCO 2002
Which competitors on the market ? • GEM • TXL • TXT
Recommended Schedules NVB 25-30 mg/m² D1, D8 + IFO 3 g/m² D1 CDDP 80 mg/m² D1 or CDDP 80 mg/m² D1 every 3 weeks every 3 weeks NP NIP during 3 to 6 cycles