Download
1 / 42
420 likes | 541 Views
Vascular Disturbances II Thrombosis and Embolism. Thromboembolic events. Activation of coagulation system Solid mass of blood constituents formed within the vasculature Thrombosis – formation of blood clot at site of coagulation system activation

E N D
Thromboembolic events • Activation of coagulation system Solid mass of blood constituents formed within the vasculature • Thrombosis – formation of blood clot at site of coagulation system activation • Embolism – migration through the vasculature to a distant site • Cause tissue damage by occlusion of blood vessels • Result in ischaemia and infarction
Thromboembolic events • ischaemia • lack of oxygen due to impaired blood supply • results in reversible cell injury or irreversible injury and necrosis (infarction) • depends on duration & tissue’s metabolic needs • infarction • tissue necrosis due to ischaemia • Major causes of morbidity & mortality • myocardial infarction, stroke, pulmonary embolism
Normal Haemostasis • Maintains blood in fluid state in normal vessels • Induces rapid, localized plug at site of vascular injury • Complex set of activators & inhibitors (procoagulant & anticoagulant influences) • 3 components • endothelium and vascular wall • platelets • proteins of coagulation and fibrinolytic cascades
Normal Haemostasis • Arteriolar vasoconstriction • Primary haemostasis temporary platelet plug a) Platelet adhesion b) Platelet activation (shape change & granule release) c) Platelet aggregation 3. Secondary haemostasis solid permanent plug a) Activation of coagulation cascade b) Conversion of fibrinogen to insoluble fibrin c) Aggregates of polymerized fibrin & platelets • Counter-regulatory mechanisms restrict plug to site of injury
Haemostatic Mechanisms - 1 • Arteriolar vasoconstriction • Exposure of subendothelial nerve fibres – reflex • Endothelial damage endothelin secretion • Primary haemostasis • Von Willebrand factor binds to exposed collagen • Platelets bind to vWF • Platelets activated on contact & release granule contents, including ADP and thromboxane (TXA2) • Platelet aggregation stimulated by ADP and TXA2 • Autocatalytic cascade of plt adhesion, activation and aggregation (ADP and TXA2)
Platelets • Glycoprotein receptors (integrins) on surface • GpIb: binds vWF important in plt adhesion • GpIIb-IIIa: binds fibrinogen important in secondary haemostasis • GpIb deficiency Bernard-Soulier syndrome • vWF deficiency von Willebrand’s disease • GpIIb-IIIa deficiency Glanzmann’s Thombasthenia • Alpha granules • Adhesion molecules (P-selectin, vWF) • Coagulation factors (fibrinogen, fibronectin, factor V and vWF) • Growth factors (PDGF, TGF-beta) • Dense bodies • ADP, ATP, calcium • Vasoactive molecules (histamine, serotonin, adrenalin) • Other enzymes • Thromboxane synthetase TXA2 Bleeding disorders
Haemostatic Mechanisms - 2 • Secondary haemostasis • Tissue factor released from damaged endothelium • Tissue factor and secreted plt factors activate coagulation cascade • Activation of thrombin • Conversion of fibrinogen to insoluble fibrin fibrin deposition • Autocatalytic activation of coagulation cascade • Binding to plt surface receptors further plt aggregation and activation • Fibrin deposition stabilizes and anchors aggregated plts
Haemostatic Mechanisms - 3 • Counter-regulatory mechanisms • Fibrinolytic pathway (Plasminogen activation formation of plasmin) • Coagulation cascade • Circulating urokinase-like plasminogen activator (u-PA) • Release of tissue-type plasminogen activator (t-PA) from endothelium • Anticoagulant pathways • Heparin-like molecules on endothelial surface antithrombin III activation • Endothelial synthesis of Protein S • Thrombin thrombomodulin activation Protein C activation • Fibrin and fibrinogen degradation • Inhibition of coagulation
Extrinsic pathway Intrinsic pathway Inhibitors Tissue factor pathway inhibitor Tissue Factor XII XI IX Collagen VII VIIa XIIa XIa IXa + VIIIa Protein C + Protein S X Xa Positive Feedback Va V Antithrombin III Prothrombin Thrombin Fibrinogen Fibrin XIII Fibrinolytic cascade Cross-linked fibrin
Thrombosis • Inappropriate activation of haemostatic mechanisms • E.g. uninjured vessel or very minor injury • Definition: • formation of solid mass of blood constituents within vascular system in life • Virchow’s triad: • changes in the vessel wall • changes in blood flow • changes in the blood constituents
Changes in the vessel wall • Primarily damage to intimal surface (endothelium) • Causes of endothelial cell injury: • ulcerated atherosclerotic plaques • scarred valves in endocarditis / prosthetic valves • radiation, cigarette smoke, cholesterol/lipids • Results of endothelial cell injury: • exposed subendothelial extracellular matrix • platelet activation • activation of coagulation cascade • depletion of antiplatelet, anticoagulant and fibrinolytic functions • endothelial activation activationof procoagulant functions
Antithrombotic functions Antiplatelet Adenosine diphosphatase ( ADP) Prostacyclin and nitric oxide (also vasodilation) Anticoagulant Heparin-like molecules (activate antithrombin III) Thrombomodulin (activates protein C) Protein S synthesis Fibrinolytic t-PA Procoagulant functions Production of vWF Production of tissue factor Binding of factors IXa and Xa Endothelium
Changes in blood flow • Normal flow is laminar • cells in centre of blood stream • clear zone of plasma adjacent to endothelium • Disrupted flow is static or turbulent • Stasis • Platelets in contact with endothelium • Prevent dilution of clotting factors • Retard inflow of clotting factor inhibitors • e.g. myocardial infarct, aneurysm, atrial fibrillation, hyperviscosity syndromes • Turbulence • Eddy currents with local pockets of stasis • Promote endothelial cell injury • e.g. ulcerated atherosclerotic plaque
Changes in blood constituents • Hypercoagulability • Leads to recurrent venous thrombosis, arterial thrombosis, recurrent abortion and stillbirths • Inherited (see table overleaf) or Acquired (below) • oral contraceptive use • pregnancy / hyperoestrogenic states • malignancy - elaboration of a procoagulant factor, leading to arterial and venous thrombosis (Trousseau’s syndrome) • tissue damage – surgery, trauma, burns • Hyperviscosity • predisposes to stasis in small vessels • polycythaemia) / deformed RBC’s (sickle cell anaemia) • Presence of endothelial cell toxins • toxins in cigarette smoke, high levels of lipid or cholesterol • predispose to endothelial cell injury
Thrombus Formation • Atherosclerotic plaque • initial fatty streak • plaque enlarges (smoking/hyperlipidaemia) • turbulence (due to protrusion into lumen) • loss of endothelium & exposure of collagen • platelet adherence & activation • fibrin meshwork deposition with RBC entrapment • more turbulence, more platelet adherence, more fibrin deposition • thrombus of alternating layers of platelets, fibrin and red blood cells
Arterial Thrombi • Large vessels (aorta, heart) - nonocclusive / mural • Smaller vessels (coronary arteries, leg arteries) - often occlusive • Classically have alternating white and red layers • called lines of Zahn • alternating layers of pale platelets and darker RBC’s • e.g. aneurysmal sacs, infarcted left ventricle, damaged heart valves, atherosclerotic plaques • Consequences: • Ischaemia in tissues distal to thrombus with possible necrosis (infarction) • May embolize due to rapid flow
Arterial Thrombi Non-occlusive thrombi in wall of atherosclerotic aorta
Arterial Thrombi Occlusive thrombus in wall of atherosclerotic coronary artery
Arterial Thrombi a b Alternating layers of a) platelets and fibrin and b) red blood cells
Venous Thrombi • Sites of stasis, commonly veins of lower extremity • Red - More enmeshed erythrocytes, less platelets • Occlusive • Predisposing factors • Bed rest, immobilization, heart failure, surgery, trauma, pregnancy, hypercoagulable states • Consequences: • Rarely cause ischaemia if affect arterial supply • More commonly embolize
Fate of Thrombi • Dissolution • by fibrinolysis • Propagation • along length of vessel complete vessel occlusion • Embolization • Recanalization • capillaries invade thrombus to re-establish blood flow • Organization • Inflammation and fibrosis replacement by scar, may obliterate vessel lumen Recent thrombi may be completely dissolved Older thrombi more resistent to fibrinolysis (extensive fibrin polymerization)
Consequences of Thrombosis • Arterial Thrombosis • Obstruction: • Myocardial infarction due to coronary artery thrombosis • Cerebral infarction (Stroke) due to carotid artery thrombosis • Acute lower limb ischaemia & infarction due to femoral/popliteal artery thrombosis • Embolization: • Cardiac/aortic mural thrombi emboli to brain, kidneys, spleen • Venous Thrombosis e.g. deep leg veins • Obstruction: • Local congestion, swelling, pain, tenderness • Oedema and impaired venous drainage • Infection & varicose ulcers • Embolization • Thrombi at or above knee pulmonary emboli
Consequences of Thrombosis Acute myocardial infarct secondary to coronary artery thrombosis
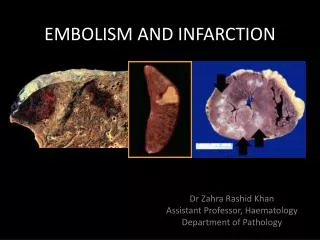
Embolism • Any intravascular mass (solid, liquid or gas) carried by blood to site distant from point of origin • Most derived from thrombi (thromboembolism) • Lodge in vessels too small to permit further passage • partial / complete vascular occlusion • distal tissue ischaemia & infarction
Pulmonary Thromboembolism • Arise from thrombi in systemic venous circulation • leg veins (95%) • pelvic veins • intracranial venous sinuses • Risk factors as for venous thrombosis • Effects are two-fold: • Possible infarction of lung tissue supplied by infarct • Interruption of oxygenation of blood within this area • Interruption of right ventricular outflow • Effects depend on size
Pulmonary Thromboembolism Embolus migrates from deep leg veins through venous system to pulmonary circulation
Pulmonary Thromboembolism Saddle embolus in branching main pulmonary artery
Pulmonary Thromboembolism Small pulmonary embolus in branch of pulmonary artery
Pulmonary Thromboembolism • Small: • silent due to collateral bronchial artery flow • organization with cumulative damage (idiopathic pulmonary hypertension) • Medium: • pulmonary infarct with acute respiratory and cardiac symptoms • Large: • right heart failure & collapse (>60% pulm circ) • Massive: • sudden death e.g. saddle embolus
Systemic Thromboembolism • Arise in arterial system (heart/large arteries) • Atheromatous plaque with thrombus • Valve vegetation • Atrial thrombus (Atrial Fibrillation) • Old myocardial infarct (adynamic) • Recent myocardial infarct (loss of endothelium) • Rarely paradoxical embolus from venous system (through septal defect in heart)
Systemic Thromboembolism • Travel in systemic circulation • Cause arterial occlusion, distal ischaemia & infarction • brain - stroke, neurological deficit / death • renal/splenic infarcts may be asymptomatic, seen as ischaemic scars at autopsy • intestine - mesenteric emboli cause intestinal infarction, can be lethal • limbs - ischaemic foot (dry gangrene)
Systemic Thromboembolism Renal infarct secondary to systemic thromboembolism
Other Forms of Embolism • Fat embolism • Next most common after thromoemboli • Fracture of long bones / Burns / Trauma • Can cause severe pulmonary insufficiency • Air embolism • Gas bubbles obstructing vascular flow • Surgical /obstetric procedures / Chest wall injury • Decompression sickness • Gases dissolve in blood at high pressure • Come out as bubbles during rapid decompression • N2 bubbles remain - muscle, jts, lungs, brain, heart
Other Forms of Embolism Fat emboli in the lung
Other Forms of Embolism • Atheromatous plaque embolism • Platelet emboli • Infective emboli (infective endocarditis) • Tumour emboli • Foreign material (talc in IVDU) • Amniotic fluid embolism • amniotic fluid forced into uterine veins @ delivery, causing respiratory distress
Other Forms of Embolism Kidney showing cholesterol embolism from an atherosclerotic plaque
Disseminated Intravascular Coagulation • Thrombotic disorder • Sudden / insidious onset of widespread fibrin thrombi in microcirculation • Diffuse circulatory insufficiency • Brain, lungs, heart, kidneys • Consumption of platelets and coagulation factors • Activation of fibrinolytic pathways • Severe bleeding disorder • Complication of any widespread activation of thrombin • Sepsis, Burns, Trauma, Extensive Surgery, Amniotic fluid embolism, Carcinoma, Intravascular haemolysis
Non-thromboembolic Vascular Insufficiency • Atheroma • M.I., hypertension due to renal artery stenosis • Spasm • angina, Raynaud’s phenomenon • External Compression • surgery, torsion, tumour • Steal syndrome • Blood diverted to one organ or tissue due to increased demands, compromising the supply of another • Hyperviscosity • Sickle cell disease splenic infarcts
Consequences of Vascular Insufficiency • Number of determining factors • Size of vessel and size of vascular territory • Partial / total vascular occlusion • Duration of ischaemia • Metabolic needs of tissue involved • Presence or absence of alternative (collateral) circulation • Most important consequence = Infarction • Commonest cause of death in western world
Summary • Thrombosis • Normal haemostatic mechanisms • Pathogenesis: Virchow’s triad • Arterial vs Venous Thrombi • Fate of Thrombi • Embolism • Types of embolus • Systemic vs Pulmonary Embolism • Other Causes of Vascular Insufficiency • Consequences of Vascular Insufficiency