Download
1 / 29
290 likes | 295 Views
This article explores the definition, causes, and burden of common mental health disorders among older people. It discusses the treatments available and the barriers they face in accessing them. The importance of an integrated view of mental and physical health is highlighted, along with the need for improved access to services for older individuals.

E N D
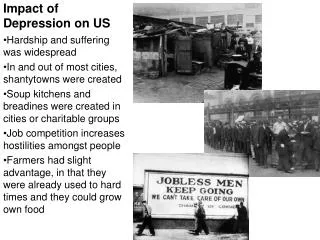
Impact of health inequalities on access to services for older people with anxiety or depression • Definition of common mental health disorders • Aetiology (causes) • Burden of Disease • Treatments • Access to treatments • Summary
What is mental health? ‘..a state of well-being in which every individual realizes his/her own potential, can cope with normal stresses of life, can work productively and fruitfully, and is able to make a contribution to her/ his community……’ WHO 2001 • Absence of mental illness • Positive mental health • Mental well-being
Dimensions of mental health If I am not for myself, who will be for me? And if I am only for myself, what am I? If not now, when? Emotional resources e.g. coping style, mood, emotional intelligence Cognitive resources e.g. learning style, knowledge, language, flexibility, innovation, creativity Mental health (capital) Meaning and purpose e.g. vision, spiritual growth, connectedness Social skills e.g. listening, relating, communicating, co operating, accepting Lynne.friedli@btopenworld.com Michael.parsonage@scmh.org.uk
Common Mental Health Disorders • Depression • Generalised anxiety disorder (GAD) • Panic disorder, phobias, social anxiety disorder • Obsessive-compulsive disorder (OCD) • Post-traumatic stress disorder (PTSD)
Serious Mental Illness • Schizophrenia • Bipolar -between 1-3 per 100
Aetiology (Causes) • Mental health and mental illnesses are determined by multiple and interacting social, psychological, and biological factors, just as health and illness in general. • Life events may act as a trigger among people who are biologically or psychologically predisposed to a disorder • Mental illness is consistently associated with deprivation, low income, unemployment, poor education, poorer physical health and increased health-risk behaviour
Particular risk factors in older people • Limited mobility, chronic pain, frailty or other mental/physical problems leading to loss of independence • Physical illness • Bereavement • Social Isolation • Loneliness
At risk older groups • Poor • ?Females ?Males • Carers • Disabled • BME • LGBT • Rural
Separate view of health Historically, mental and physical health have been seen as separate and non- interacting domains, resulting in separate treatment approaches and policies Mental Health Physical Health
An integrated view of health In reality, there is considerable overlap and interaction between physical and mental health Poor mental health is probably a larger contributor to health risk behaviours and poor physical health than the other way round Physical Health Mental Health
Inter relationship between mental and physical health • Mental health is a key factor in the adoption and maintenance of unhealthy lifestyles • Mental health problems increase the risk of premature mortality from diseases such as cardiovascular disease • Physical health problems can affect mental health
The latest mid-2012 population counts are: Over the next 10 years, the pop of over 65s in England will increase by 15%, and the over 85s by 27 %. By 2035, the number of people aged 85 and over is projected to be almost 2½ times larger than in 2010. The population aged 65 and over will account for 23% of the total population in 2035.
Treatment in older people • Antidepressants • Talking Therapies: • Good evidence base for the management of depression in older people • IAPT data indicates there is no difference in recovery rates for those aged over 64 year • Older people like/prefer talking therapies
Where treated • Mainly in general practice • In i year, 38% of people with a CMHD contacted their GP for help • Of the 130 cases of depression (including mild cases) per 1000 population, 80 consult their GP but 49 not recognised as depressed • Access to IAPT for older people was 5.2% compared to 12% target set out in the ‘Talking therapies: four year plan of action’
Why lower rates of treatment in older people? • Patient factors • Practitioner-level factors • System- and service-level factors • Resource-based or practical factors
1. Patient Factors • Feelings of shame • Stigma and fear • Distrust of healthcare services • Masking and normalising of symptoms • Lack of knowledge about mental health symptoms or services • Lack of support or encouragement to access healthcare services from families and community • Belief in spirituality and self-reliance as a means of overcoming healthcare problem • Somatisation
2. Practitioner Factors • Lack skills to identify/manage CMHD in older people • Inadequate assessments arising from limited information about a range of issues e.g. cultural background • Minimisation/poor recognition of MH symptoms • Attribute CMHD symptoms to patient’s reactions to physical health problems e.g. diabetes, Parkinson’s disease etc • Poor attitude to patients and mental illness e.g. consider that depression is an inevitable consequence of ageing and fail to see the value of treating it • Believe that treating physical health problems is higher priority than treating mental health problems, • Mistakenly believe that psychological therapies do not work for older people • Prioritise referring younger people with CM • Time constraints
2. Practitioner contd • Recognise symptoms of CMHD but fail to realise that they can be treated with psychological therapies • HD
System- and service-level factors • Poor allocation of services and poor quality of services • Poor communication between services • Lack of flexibility in healthcare systems and practices to take into account individuals’ cultural beliefs • Use of standard procedures and practices that are unfamiliar or unexplained to vulnerable individuals
Resource-based or practical factors • Transportation issues • Poor appointment systems
Summary Common mental health disorder (CMHD) in older people • As common in older people as in younger • Results in significant disease burden including impact on co-existing physical illness • Is under-recognised and under-acknowledged and undertreated • Worse in certain sub-groups: men, BME, LGBT
Relationship between levels of prevention, intensity of intervention, mental illness, recovery and well-being Mental illness Recovery treatment & tertiary intervention Early signs of illness early intervention & secondary prevention High risk groups including history of mental illness secondary prevention General population Primary prevention Increasing levels of well-being
Create flourishing, connected communities A Public Mental Health Framework for Developing Well-Being Meaning from adversity: • Post traumatic growth • Psychological therapies • Positive reflection Promote meaning & purpose Cultivate purposefulness & fulfilment: • In life, work, education and volunteering • By creativity, coherence and flow • With inclusive beliefs and values Enhance: • Community engagement • Ecological intelligence and connectedness Reduce social exclusion: • Address discrimination and stigma • Target high risk groups Develop sustainable, connected communities Integrate physical & mental health & well-being Improve: • Physical activity • Healthy Food • Sexual Health • Health Checks Reduce: • Smoking • Alcohol • Drugs • Obesity Reduce risk factors Promote protective factors Reduce Inequalities: • Unemployment • Fuel Poverty • Homelessness • Violence and Abuse • Impact of Climate Change Promote: • Employment • Benefits Checks • Safe Green Spaces • Insulated & Warm Homes • Partnership Working Build resilience & a safe, secure base Prevent and reduce impact of Adverse Childhood Experiences: • Child abuse • Parental mental illness • Parental substance misuse • Parental Domestic Abuse • Household offender • Childhood bereavement Improve: Parenting & Parental Health • Social and Emotional Literacy in Healthy Schools • Early interventions for conduct & emotional disorders Ensure a positive start in life Nurse J 2008
The effect of shifting the mean of the mental health spectrum From: Huppert Ch.12 in Huppert et al. (Eds) The Science of Well-being Flourishing Moderate mental health Mental disorder Languishing Number of symptoms or risk factors
Thank You Mike.mchugh@leics.gov.uk