Download
1 / 19
210 likes | 285 Views
Sensory Lesions. Dr. ZAHOOR ALI SHAIKH. Peripheral Neuropathy 1. Polyneuritis or Polyneuropathy (When many peripheral nerves are affected) All forms of sensations are impaired in distal parts of limbs (Glove & stocking anesthesia) Usually symmetrical. Polyneuritis or Polyneuropathy 2.

E N D
Sensory Lesions Dr. ZAHOOR ALI SHAIKH
Peripheral Neuropathy 1 • Polyneuritis or Polyneuropathy (When many peripheral nerves are affected) All forms of sensations are impaired in distal parts of limbs (Glove & stocking anesthesia) • Usually symmetrical
Polyneuritis or Polyneuropathy 2 • Causes : Diabetes Mellitus, Vit. B deficiency (B1, B6, B12) Drugs e.g. INH (anti T.B.) • Patient complaints of, numbness, sometimes pain in the feet • On examination: loss of position & vibration sense.
Herpes Zoster • This disease results from reactivation of the varicella virus which has lain dormant in posterior root ganglia following chickenpox infection earlier in life . • Why reactivation? Usually when body resistance is decreasd.e.g. Steriod therapy, Leukemias, • The first symptom is severe , continuous pain in the dermatomal distribution of the affected nerve root . (nerve root distribution.) • After 3-4 days the skin becomes red and vesicles appear in the affected area . • These vesicles dry up in 5-6 days , and the pain subsides . • Sometimes small scars and anesthesia remains in the affected segment
Dermatomes of Spinal roots & Divisions of Trigeminal (V) nerve
Tabes Dorsalis (1) • Is a form of Neurosyphilis ( syphilis is a sexually-transmitted disease , STD). • It can cause damage to the dorsal root, and dorsal ( posterior ) columns . Consequently , there will be : (1) impairment or loss of proprioception ( vibration , position senses ) and two-point discrimination sense . (2) Absent tendon jerks . Explain why ?
Tabes Dorsalis (2) (3) Sensory ataxia ( ataxia means loss of coordinated muscular contractions required for the production of smooth movements) . Expalin why ? • Q: How do we ascertain the presence of sensory ataxia ? A : By performing Romberg’s Test . In a patient with damaged psterior columns of the spinal cord we get a +ve Romberg Test . A positive Romberg’s Test (Sign) : means that keeping the feet together , the patient can stand steadily with the eyes open ; but if he closes his eyes he become unsteady and tends to fall . Explain why ? • Gait : wide based & stamping gait. Why?
Brown –Sequard Syndrome (1)(Hemisection of spinal cord) • Causes: due to stab injury , gunshot ( bullet ) wound, or tumor . • The example shown here is a lesion on the left side at the thoracic level of the spinal cord : • Ipsilaterally ( on the same side of lesion ) • At the level of the lesion : Loss of all sensations. • Below the level of the lesion : loss of vibration , position and two-point discrimination . Why ? • Contra laterally (on the opposite side ) : loss of pain and temperature sensibility Why ?
Brown-Sequard Syndrome Site of Lesion
There is motor weakness ( lower motor neuron type at the level of the lesion. Below the lesion- Spastic lower limb (with upper motor neuron type of lesion on the same side). Why ? Brown –Sequard Syndrome (2)
Syringomyelia (1) • This disease is due to presence of one or more cysts ( fluid-filled cavities , called syrinx ) near the central canal of the spinal cord. • The expanding cysts damage second-order spinothalamic fibers which cross directly in front of the central canal , affecting pain & temperature fibers on both sides at the affected segment • The loss of pain and temperature sensations extends to several segmental levels . Therefore , we get Segmental Loss of pain and temperature sensations .
However , the patient retains touch and pressure sense as well as vibration and position sensations (why are they spared ?) This selective loss of pain and temperature while sparing touch and proprioception is called Dissociated sensory Loss ( or Dissiciated Anesthesia) Syringomyelia (2) Loss of pain and temperature sensation
The Parietal Lobe is an Essential Component of the Somatosensory System • And because its post-central gyrus receives afferent pathways for perception (appreciation ) of body position and touch , damage to S1 leads to loss of : • (1) Ability to accurately localize light touch • (2) Two-point discrimination • (3) Ability to appreciate size , shape , texture and weight of objects (without looking at them) Stereognosis • Sensory inattention ( & hemineglect ) Amorphosynthesis occur due to damage to somatosensory association area, as this area plays important role in interpreting the meaning of sensations perceived by main sensory area S1
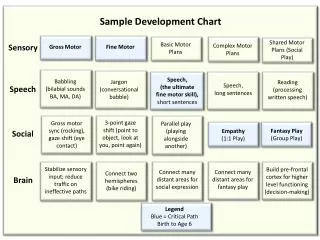
(a) Thalamic (b) Mid-brainstem
Weak (UMN) (c) Central Cord (d) Unilateral cord lesion (Brown-Sequard)
(e) Transverse thoracic spinal cord (f) Dorsal column
T5 C6 L4 (g) Sensory roots (h) Polyneuropathy
Principal patterns of loss of sensation -- T5 - C6 - UMN --- L4 (a) (b) (c) (d) (e) (f) (g) (h) • Thalamic lesion: sensory loss throughout opposite side. • Brainstem lesion (rare): contralateral sensory loss below face and ipsilateral loss on face. • Central cord lesion, e.g. syrinx: ‘suspended’ areas of loss, often asymmetrical and ‘dissociated’, i.e. pain and temperature loss but light touch remaining intact. • ‘Hemisection’ of cord or unilateral cord lesion=Brown-Sequard syndrome: contralateral spinothalamic (pain and temperature) loss with ipsilateral weakness and dorsal column loss below lesion, UMN, upper motor neurone. • Transverse cord lesion: loss of all modalities below lesion. • Isolated dorsal column lesion, e.g. demyelination: loss of proprioception, vibration and light touch. • Individual sensory root lesions, e.g. C6 (cervical root compression), T5 (shingles), L4 (lumbar root compression). • Polyneuropathy: distal sensory loss.