Download
1 / 40
400 likes | 407 Views
Newborn Screening and Children’s Special Health Care Services. Lois Turbett, MS, RN Nurse Consultant. Purpose of Newborn Screening (NBS). Early diagnosis Early treatment Reduce morbidity and mortality Reduce financial burden. 50 th Anniversary of NBS.

E N D
Newborn Screening and Children’s Special Health Care Services Lois Turbett, MS, RN Nurse Consultant
Purpose of Newborn Screening (NBS) • Early diagnosis • Early treatment • Reduce morbidity and mortality • Reduce financial burden
50th Anniversary of NBS • Robert Guthrie publishes A Simple Phenylalanine Method for Detecting Phenylketonuria in Large Populations of Newborn Infants. Pediatrics 1963; 32:338-342 • 1963 Massachusetts becomes the first state to mandate screening for phenylketonuria (PKU) in newborns
Early History of Michigan NBS • 1965 PKU • 1977 congenital hypothyroidism (CH) • 1985 galactosemia • 1987 biotinidase deficiency, maple sugar urine disease (MSUD) and hemoglobinopathies • 1993 congenital adrenal hyperplasia (CAH) • 2003-2005 additional metabolic disorders • 2007 cystic fibrosis (CF) • 2011 severe combined immunodeficiencies (SCID)
217 Babies Diagnosed through NBS in 2011 • Cystic fibrosis (13) • Endocrine (86) • Congenital hypothyroidism (78) • Congenital adrenal hyperplasia (8) • Hemoglobinopathies (61) • Metabolic disorders (57) • Primary immunodeficiencies (0)
Michigan Compiled LawsSection 333.5431 • Mandated • Hospitals • Birthing attendants (midwives) • Parents may opt out • Rare • Fax signed refusal form to NBS Follow-up • 517-335-9419 or • 517-335-9739
NBS Results • Faxed to the primary care provider (PCP) listed on the NBS card • Consult with medical management centers as needed • Explain to family meaning of screen • Arrange with family for a repeat newborn screen when requested
NBS Results on MCIR • NBS results are posted on Michigan Care Improvement Registry (MCIR) • Click on “Newborn Screening Tab” • Click on “Results” (opens PDF) • Primary care offices have access; local health departments (LHDs) usually do not
Role of LHD CSHCS • Know the disorders-more than a “PKU test” • Cystic fibrosis • Endocrine • Hemoglobinopathies • Metabolic • Primary immunodeficiencies • 50+ disorders screened as well as hearing
NBS Results • Normal • Inconclusive and borderline • Fax report to management center • Fax report to primary care provider (PCP) • NBS Follow-up requests repeat screen
Role of LHD CSHCS,Borderline Positive (B+) • NBS referral sent to LHD via EZ Link • Check to see if family due in for WIC • Check to see if enrolled in Maternal Infant Health Program (MIHP) • Call family • Visit if in the neighborhood • Assist family to obtain a primary care provider (PCP) for infant • Obtain repeat screen at a local birthing hospital
NBS Results (cont.) • Strong positive • Fax report to PCP • Fax report to management center; assure referral received • Management center assumes follow-up of strong positive referral
Role of LHD CSHCS, Strong Positive (S+) • CSHCS diagnostic referral • All NBS diagnoses are covered by CSHCS • Sub-specialist referral depends on the disorder
Medical Management Centers • Newborn Screening and Coordinating Program for Cystic Fibrosis (University of Michigan) • Newborn Screening Endocrine Follow-up Program (University of Michigan) • Sickle Cell Disease Association of America, Michigan Chapter • Children’s Hospital of Michigan Metabolic Clinic • Children’s Hospital of Michigan Coordinating Center for Primary Immunodeficiencies
Cystic Fibrosis (CF) • High immunoreactivetrypsinogen (IRT) • Enzyme created by the pancreas • High in infants with CF • Other conditions can also cause elevation • Mutation for Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) • Michigan tests for 40 common mutations
Cystic Fibrosis (CF) (cont.) • High IRT, no mutation • Primary care provider (PCP) notified • PCP to monitor health status of infant • High IRT, one or two mutations • Referral to management center • Arrange for sweat chloride test • Notify NBS follow-up if the mother of a CSHCS CF client is pregnant
Role of LHD CSHCS,S+ CF • CSHCS diagnostic referral to a certified CF center for sweat test • Helen DeVos Children’s Hospital • Western Michigan University, Kalamazoo • Michigan State University, Lansing • Mott (Ann Arbor & Flint) • Children’s Hospital of Michigan • Toledo (borderland)
Congenital Hypothyroidism (CH) • Test for thyroid stimulating hormone (TSH) • Cutoffs vary depending on age • Untreated CH may lead to irreversible decreased intellectual ability
Role of LHD CSHCSS+ CH • Medical management center refers to pediatric endocrinologist for serum TSH and serum free T4 • CSHCS diagnostic referral if indicated • Insurance prior authorization for Synthroid instead of levothyroxine
Congenital Adrenal Hyperplasia (CAH) • 17-hydroxyprogesterone (17-OPH) • Newborn may already show signs of CAH while in the hospital • Ambiguous genitalia (female) • Clinical picture
Role of LHD CSHCSS+ CAH • Immediate referral to pediatric endocrinologist • CSHCS diagnostic referral • Retroactive diagnostic • CSHCS backdating • CSHCS nurse should assure family understanding of written emergency plan for CAH
Hemoglobinopathies • Sickle cell anemia • β thalassemia • Sickle β thalassemia • Hb H disease ( thalassemia)
Role of LHD CSHCS Hemoglobinopathies • CSHCS diagnostic referral • Be familiar with pain management challenges • Ask to see the patient’s notebook • Transition to adult Hem/Onc
Metabolic Disorders • Amino acid disorders • Fatty acid disorders • Organic acid disorders • Other disorders
Amino Acid Disorders • Phenylketonuria (PKU) • Classic PKU • Non-PKU hyperphenylalanemia • Maple sugar urine disease (MSUD) • Arginosuccinic acidemia (ASA) • Citrullinemia type I (CIT-I) • Arginase deficiency (ARG) • Citrullinemia type II (CIT-II)
Fatty Acid Disorders • Carnitine uptake defect (CUD) • Medium-chain acyl-CoA dehydrogenase deficiency (MCAD) • Very long-chain acyl-CoA dehydrogenase deficiency (VLCAD)
Organic Acid Disorders • 2MBG - 2-Methylbutyryrl-CoA dehydrogenase deficiency • Isovaleric acidemia (IVA) • Glutaric acidemia Type I
Other Disorders • Classic galactosemia • Life threatening • Immediate switch to soy formula; discontinue breastfeeding • Duarte galactosemia • Mild, often no treatment • Biotinidase deficiency • Treated with daily biotin
Role of LHD CSHCSMetabolic Disorders • Know the disorder for your enrolled child • Many disorders can be life threatening; others are mild • Assure family understanding of written emergency plan • Access to care issues • Detroit, Grand Rapids, Ann Arbor
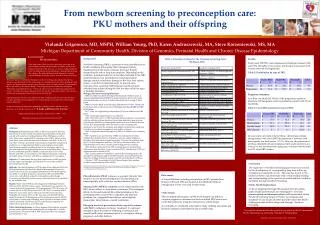
Role of LHD CSHCSMetabolic Disorders • Prior authorization challenges for metabolic formula • Lifetime PKU diet • Maternal PKU • May need to get mom back on CSHCS if pregnant and <21 • Baby can develop permanent intellectual impairment if mother does not follow diet
Severe Combined Immunodeficiency (SCID) • A group of inherited disorders characterized by the lack of a functioning immune system • “Combined” defect in both T and B-cell function • Exposure to common illnesses and live vaccines is life threatening
NBS SCID Testing • Test for T-cell receptor excision circles (TRECs) • By-product generated during T-cell development • Low or absent number means infant is not making T-cells • Michigan began testing for SCID October 3, 2011
Role of LHD CSHCSPrimary Immunodeficiencies • Diagnostic referral, flow cytometry • DeVos • University of Michigan • Children’s Hospital of Michigan • If true SCID, bone marrow transplant (BMT) is likely • May need intravenous immune globulin (IVIG) until BMT
Recap • B+, repeat newborn screen needed • S+, CSHCS diagnostic referral • Confirmed case, CSHCS eligible
NBS Newsletter Online • www.michigan.gov/newbornscreening
NBS Information • 866-673-9939 • Fax 517-335-9419 • newbornscreening@michigan.gov • www.michigan.gov/newbornscreening • www.michigan.gov/biotrust • Lois Turbett • turbettl@michigan.gov • 517-335-1966