Download
1 / 35
370 likes | 423 Views
Management of traumatic injuries. I ntroduction.

E N D
Introduction • Traumatic injuries can occur at any age but most commonly they are seen at the age of 2-5 years during which children are learning to walk. Another age at which dental injuries are common is 8-12 years when there is increased sports activity, and while learning bicycle, etc.
Etiology of Traumatic Injuries • Automobile injury • Battered child • Child abuse • Drug abuse • Epilepsy • Fall from height • Sports related injuries
post normal occlusion overjet exceeding 4mm short upper lip incompetent lips mouth breathing (Forsberg & Tedestam) Predisposing factors
Sex and age distribution -boys > girls (2:1) -first two decades of life (8-12yrs) Susceptible tooth -maxillary central incisor(80%) -maxillary lateral incisor -mandibular central and lateral incisors Comparison of injuries to primary and permanent teeth -trauma to primary dentition confined to supporting structure -trauma to permanent dentition represented by crown fractures Incidence
Energy of the impact Resilience of the impacting object Shape of the impacting object Direction of the impacting force Factors characterizing an impact to the teeth
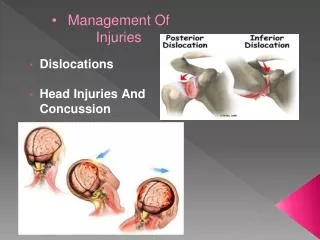
CLASSIFICATION OF DENTOFACIAL INJURIES Soft tissue injury • Ulceration Abrasion Contusion Laceration injury • Concussion • Subluxation intrusive luxation • Lateral luxation • Extrusive luxation • Avulsion Tooth fractures: • Enamel fractures • Uncomplicated crown fracture • Complicated crown fracture • Crown-root fracture Root fracture Facial skeletal injury • Alveolar process body of mandible TMJ
Class I -Fracture involving enamel Class II -Fracture involving enamel & dentin Class III -Fracture involving enamel,dentin & pulp Class IV -Teeth that lost their vitality with or without loss of crown Class V -Traumatically avulsed tooth Class VI -Fracture of the root with or without crown fracture Class VII -Displacement of the tooth without crown/root fracture Class VIII -Cervical crown fracture Class IX -Fracture of deciduous teeth Ellis and Davey’s classification (1970)
History of the accident - when? - how? - where? Clinical examination -neurologic examination History and clinical examination • Chief complaint
Notice unusual communication or motor functions Look for normal respiration without obstruction of the airway or danger of aspiration Replant avulsed teeth as indicated Obtain a medical history and information on the accident Determine blood-pressure and pulse Examine for rhinorrhea or otorrhea Evaluate function of the eyes- Is diplopia or nystagmus apparent? Are pupillary activity and movement of the eyes normal? Out line of initial neurologic assesment (Croll TP et al )
6. Evaluate movement of the neck for pain or limitation. 7. Examine the sensitivity of the facial skin for paraesthesia or anesthesia 8. Confirm normal vocal functions 9. Confirm patient’s ability to protrude the tongue 10. Confirm hearing (tinnitus or vertigo) 11. Evaluate sense of smell 12. Ensure follow up evaluation
Allergic reaction to medication Systemic disorders Current medications Tetanus immunization status Medical history
Inspection –laceration, swelling or bruising of the face, cheek, neck or lips Palpation – TMJ, zygomatic arch, angle & lower border of the mandible External examination
Soft tissue Inspection of the tongue, oral mucosa, palate, floor of the mouth & gingiva for lacerations Palpation of the oral mucosa, facial & lingual gingivae, anterior border of the ramus of the mandible for areas of tenderness, swelling or bruises. Intra oral examination
Hard tissue Allignment of teeth Mobility of teeth -alveolar fracture -displacement -coronal fracture of the crown -root fracture -incomplete cusp fracture(tooth slooth)
Traumatized teeth vulnerable to false negative reading. Thermal test- heated gutta percha, ice, CO2snow sticks. Electric pulp tests Performed at the time of initial examination, 3weeks, 3, 6, 12months & at yearly intervals to establish a physiologic status of the pulp. Laser doppler flowmetry Vitality test
One occlusal exposure (gives an excellent view of lateral luxation, alveolar fracture, apical and mid root fracture) + Three periapical bisecting angle exposures (horizontal fracture & displacement of the tooth) Extra oral radiography Radiographic Examination
Photographic registration of trauma Exact documentation -treatment planning -legal claims -clinical research
Crown infraction - Incomplete fracture of the enamel without loss of tooth structure. - Microcracks in the thickness of enamel - Rarely occurs alone and can be sign of attachment injury
Diagnosis - observed during routine examination - detected using indirect light or transillumination -use of dyes Treatment • Infracted tooth does not require treatment but vitality tests are necessary to determine extent of pulp damage. • Smoothening of rough edges by selectively grinding of enamel
Repairing fractured tooth surface by composite if needed for cosmetic purposes • Regular pulp testing should be done and recorded for future reference. • Follow-up of patient at 3, 6 and 12 months interval is done. Prognosis: good
Crown fracture Uncomplicated Crown Fracture • Crown facture involving enamel and dentin and not the pulp is called as uncomplicated crown fracture . Pulp may remain normal or may get chronically inflamed depending upon proximity of fracture to the pulp, size of dentinal tubules and time of the treatment provided. Diagnosis • It could be easily revealed by clinical examination. If dentin is exposed, sensitivity to heat or cold may be present. Treatment • The main objective of the treatment is to protect the pulp by obliterating dentinal tubules. • In case of enamel fractures, scJccth c grinding of incisal edges will be sufficient to remove the sharp edges to prevent injury to lips, tongue, etc.
If there is involvement of both enamel and dentin • A restoration is needed to seal the dentinal tubules and to restore the esthetics. Dentinal tubules can also be sealed with zinc oxide eugenol cement, glass ionomer cement or dentin bonding agent. • If the fracture fragment of crown is available, reattach it • Following techniques are employed for reattachment of fractured fragment. • Bevelling of enamel: • internal dentinal groove • Internal enamel groove • Over contouring: In this technique after joining fractured fragment, a composite layer of 0.3 mm is placed superficially on buccal surface.
Prognosis • Patient should be recalled and sensitivity testing is done at the regular interval of 3, 6 and 12 months. Prognosis is good.
Enamel-dentin fracture with pulpal involvement (complicated crown fracture) -Involves enamel, dentin & pulp -Diagnosis - clinical examination of the tooth - pulp exposure - tooth is sensitive to variation in temperature,dehydration and pressure -vitality test is positive unless there is concomitant luxation injury -Incidence -2-13% of all dental injury
Treatment Treatment of pulp exposure • vital pulp therapy -pulp capping -partial pulpotomy -cervical pulpotomy • pulpectomy Pulp capping Pulpotomy
Choice of treatment -time spent with the exposed pulp -health of the pulp before trauma -diameter of the pulp exposure -age of the tooth -concomitant luxation injury -stage of root development Prognosis -pulp capping- pulp survival varies from 63-88% -partial pulpotomy- pulp survival varies from 94-100% Treatment of the fractured tooth -composite restoration -fragment bonding
Crown and root fracture -Involves enamel, dentin,and cementum -Pulp may or may not be involved -Fracture extends below the cemento-enamel junction Diagnosis and clinical presentation - chisel type of fracture with a fragment or fragments below the lingual gingiva - fragment may be firm, loose and attatched only to the periodontal ligament or may be lost - periodontal injury causes pain on pressure or biting - exposed dentin or pulp causes sensitivity to variation in temperature, dehydration and pressure Incidence - 5% of all dental injuries
Treatment • The primary goal of the treatment is the elimination of pain which is mainly because of mobile crown fragment The main objective of the treatment is to: • a. Allow subgingival portion of the fracture to heal. • b. Restoration of the coronal portion.
Following should be considered while management of crown root fracture: • • If there is no pulp exposure, fragment can be treated by bonding alone or by removing the coronal structure and then restoring it with composites
If pulp exposure has occurred, pulpotomy or root canal treatment is indicated depending upon condition of the tooth. • When remaining tooth structure is adequate for retention, endodontic therapy and crown restoration are possible with the help of crown lengthening procedures • When root portion is long enough to accommodate a post retained crown, then surgically removal of the coronal fragment and surgical extrusion of the root segment is done • To accommodate a post retained crown, after removal of the crown portion, orthodontic extrusion of root can also be done
Root fracture Fracture of cementum and dentin involving the pulp Mechanism- Frontal impact creates a compression zones labially and lingually and the resulting shearing stress zone dictates the plane of fracture.
Incidence : relatively infrequent occurs in less than 3% of all dental injuries Diagnosis and clinical presentation The extent of displacement of the coronal segment is usually indicative of the location of the fracture and can vary from simulating a concussion injury (apical fracture ) to simulating an extrusive luxation (cervical fracture) Radiographic examination Imperative to take 3 angled radiographs Central beam is directed with a maximum range of 15-20o of the fractured plane Treatment Emergency treatment involves repositioning of the segments in as close proximity as possible and rigidly splinting to adjacent teeth for 2-4 months
if coronal pulp becomes non vital In such cases following treatment options are avalable • Rct for both coronal and apical segment • Rct for coronal segment and no treatment for apical segment • Rct for coronal segment and surgical removal for apical segment • Apexification • Intraradicular splinting
Prognosis:depends on • Amount of dislocation and degree of mobility of enamel • Stage of tooth development