Download
1 / 50
500 likes | 833 Views
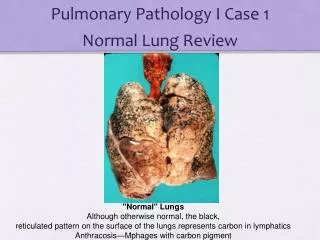
Pathology of the Lung Pneumonias. Pulmonary Infections. • More frequent than infections of any other organ. • Majority are upper respiratory tract. infections caused by viruses (common cold, pharyngitis ). • Lower respiratory infections can be.

E N D
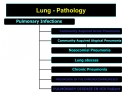
Pulmonary Infections • More frequent than infections of any otherorgan • Majority are upper respiratory tract infections caused by viruses (commoncold, pharyngitis) • Lower respiratory infections can be bacterial, viral, mycoplasmal and fungallung infections (pneumonias) • Pneumonias account for much morbidity& are responsible for 1/6 of all US deaths
Pneumonia • Broadly defined as any infection ofthe lung parenchyma • Another term is pneumonitis
Lung- defense mechanisms • Immune opsonins (alveolarmacrophages) • C3b, IgA, IgG • T lymphocytes normally in airspaces • Neutrophils (not normal), easilyrecruited
Lung- Clearing mechanisms interfered with • Injury to Mucociliary apparatus(cigarette smoke, inhaling hot or corrosive gases, viral diseases, genetic disturbances) • Loss of Cough reflex (comma, anesthesia, neuromuscular disorders, drugs, chest pain) • Interference with phagocytic or bacterial action of alveolar macrophages (alcohol, tobacco smoke, anoxia, oxygen intoxication) • Pulmonary congestion and edema • Accumulation of secretions (cystic fibrosis, bronchial obstruction)
Clinical - pneumonia • Abrupt high fever, cough, rusty purulent sputum • Chest pain, pleural rub (if there ispleuritis) • Decreased air entry, consolidation, X- ray •Sputum Microscopy, gram stain ,culture And sensitivity.
Pneumonia-classifications • Primary/Secondary, Acute/Chronic,Necrotizing, • Mode of infection- community acquired, hospital acquired/nosocomial, aspiration • Site of action- alveolar space (typical), alveolar wall (atypical) • Microorganism- Bacterial, Viral, Chlamydia, Fungi etc
Pneumonia-classifications • Off course the age-old classification based on Anatomy and radiological appearance: -Lobar pneumonia -Bronchopneumonia
Secondary pneumonia Underlying abnormality predisposes - Postoperative (ventilation reduced) - Smoking (mucociliary reflex) – Aspiration (due to loss of cough andswallowing reflex) -Preexisting lung disease - viral infection, emphysema, bronchiectasis -Immunosuppression
Secondary pneumonia - contd. - Bronchial obstruction-tumor, foreign bodies - Coma - cough reflex lost– Alcoholics, diabetes
Pneumonia Syndromes (7) • Community-Acquired - Acute Pneumonias - Atypical Pneumonias • Hospital acquired/Health care acquired* • Aspiration Pneumonias • Chronic pneumonias • Necrotizing Pneumonias and Lung Abscess • Pneumonia in the immunocompromised hosts * Nursing home, rehabilitation centers
The Pneumonia Syndromes Community acquired Acute Pneumonia Healthy person/Virulent organism Strep. pneumonia, Hemophilus, Moraxella, Staph, L. pneumophilia,Klebsiella and Psuedomonas Atypical pneumonia Mycoplasma, Chlamydia, CoxiellaBurnetti, and viruses (influenza)
The Pneumonia Syndromes Hospital/Heath care facility Acquired Pneumonias •Nosocomial -Gram negative rods belonging toEnterobacteriaceac-Klebsiella,E.coli, Pseudomonas - Staph Aureus (MRSA) -Immunosuppression, antibiotics,catheters, ventilators
The Pneumonia Syndromes Aspiration pneumonias • Acid Occur in those who aspirate gastric contents(either while unconscious or by vomiting) Frequent cause of death - those who survive,a common complication is lung abscessformation • Mixed nature of organisms • Anaerobic oral flora and Aerobicorganisms
The Pneumonia Syndromes Aspiration Pneumonia -Anerobic oral flora -Bacteroides, Fusobacterium,Peptostreptococcus -Aerobic -Strep, Staph, H. Influenzae, Pseudomonas
The Pneumonia Syndromes Chronic Pneumonia Nocardia Actinomyces Granulomatous MTB, Atypical MycobacteriumFungal Histoplasma,Coccidioides,Blastomyces
The Pneumonia Syndromes Necrotizing Pneumonia and LungAbscess -Anaerobic(extremely common) -Staph Aureus, , Klebsiella,Streptococcus pyogenes
Case 1 • 48 yr male presents with a mass lesion in his left lower lobe • Clinical diagnosis malignancy • Wedge resection is performed
Diagnosis • Frozen section diagnosis Necrotic tissue; no tumor seen • Final diagnosis - Tuberculosis of Lung - Special stains for Acid fast bacilli werepositive
Case 2 • 19 year old with a bronchoscopic biopsy of a lung lesion
Diagnosis •Granulomatous inflammation • Accompanying bronchial washingsshowed 4 + acid fast bacilli
Case 3 • 47 yr female with bilateral interstitial lung infiltrates
Diagnosis • Pneumocystis Pneumonia
Case 4 • 55yr old with bilateral lung disease, unknown etiology
Diagnosis • Acute Bronchopneumonia
Pneumonia • Site of action- • alveolar spacebacterial • alveolar wallatypical viral
Lobar Pneumonia • Large confluent areas of consolidation • Almost whole lobe • Bronchi not involved • Spread through pores of Kohn • Usually virulent organism- Strep. pneumonia
Bronchopneumonia: • bronchi + surrounding alveoli • Patchy • Usually less virulent organisms • bronchi, bronchioles also damaged • intervening areas normal • less chances of pleuritis
Pneumonia: stages • Both lobar and broncho pneumoniago through 4 stages if untreated • Antibiotics halt the process
Acute Congestion • heavy red boggy lungs • bacteria multiply in alveoli, dilated alveolar capillaries,early fluid exudation • early PMNs + early red cells
Red Hepatization • consistency liver like • lining alveolar cells lost • PMNs, fibrin, red cells ±Pleuritis • infection controlled
Gray hepatization • dry, gray, firm • exudation andhyperemia stop • red cells depleted
Resolution • Removal of exudate • complete resolution can occur because structure of alveoli notdamaged in lobar pneumonia • Bronchopneumonia has structural damage
Complications of pneumonia • Pleural effusion • Lung abscess: anaerobic bacteria,Staphylococcus aureus, Klebsiellapneumoniae, Streptococcuspyogenes •Empyema • Meningitis, bacteremia, endocarditis,arthritis
Lung Abscess • Copious, foul sputum, hemoptysis,fever, malaise • Complications - bronchopleural fistula, empyema, septicemia,amyloidosis • Treat with antibiotics
Pseudomonas aeroginosa • Cystic fibrosis •Nosocomial, neutropenic patients, burns •Vasculitisand vascular spread •Psuedomonassepticemia is a veryfulminant disease
Staph. aureus pneumonia: • After viral respiratory illness -secondary •Nosocomial (MRSA Penicillinresistance) • Abscess formation, empyema • I/V drug abusers- endocarditis
Klebsiella Pneumonia • Most frequent gram negative pneumonia • Debilitated and malnourished • Chronic alcoholics • Thick gelatinous sputum ( viscid capsular material) • Extensive destruction
H. Influenzae pneumonia • After viral respiratory illness - secondary • Common cause of community acquiredpneumonia in adults • With routine use of the vaccine, theincidence of disease caused by the bserotype has decreased significantly • Can cause endocarditis • Most common cause of acuteexacerbation of COPD
Moraxellacatarrhalis • Elderly individuals • Second most common cause of pneumonia in COPD •Otitis media in children
Pneumococcal pneumonia • Settings- Healthy young adult,Post viral infection, CHF, COPD, immune deficiency, splenectomy (auto) • Sputum - gram positive diplococci- lookfor intracellular organism within neutrophils. • Blood culture - more specific •Vaccines for patient in susceptible groups.
Legionella pneumonia • Sporadic, epidemic • Artificial water pools- tubing, cooling towers •In chronically ill patients, post transplant • High fatality • Culture- best for diagnosis, others- sputum, urine
Downloaded from: StudentConsult (on 13 January 2012 01:01 PM)