Download
1 / 47
530 likes | 788 Views
Peripheral Vascular System& lymphatic system. Introduction. Vascular system consists of vessels of body; any disease in vascular system creates problems with delivery of O2 & nutrients to tissues/elimination of waste products from cellular metabolism. - Arteries:.

E N D
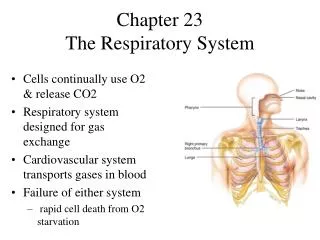
Introduction • Vascular system consists of vessels of body; any disease in vascular system creates problems with delivery of O2 & nutrients to tissues/elimination of waste products from cellular metabolism.
- Arteries: • artery walls are strong, tough & tense to withstand pressure demands. Stretch with systole& recoil with diastole, vascular smooth muscle VSM contracts or dilates which changes the diameter of arteries to control the rate of blood flow. Each heart beat creates a pressure wave which makes arteries expand then recoil, recoil propels blood through like a wave or pulse, you can feel it only at body sites where the artery lies close to skin & over bone.
1) Temporal artery • 2) Carotid artery • 3) Arteries in arm: brachial artery bifurcates into ulnar & radial artery__ superficial & deep arches • 4) Arteries in legs: femoral- popliteal- dorsalis pedis- posterior tibial.
-Veins: • its parallels arteries, but we have more veins lies closer to skin. • 1) Jugular veins • 2) Arm veins: superficial & deep • 3) Legs veins: 3 types: • 1- Deep veins: alongside deep arteries & conduct most of venous return from legs- femoral & popliteal veins • 2- Superficial veins: saphenous veins • 3- Perforators: connecting veins, have valves
* Venous Flow: • drain deoxygenated blood & waste from tissue & return to heart. A low pressure system, don’t have a pump system to generate blood flow need mechanism to keep blood moving, this accomplished by: • 1- contracting skeletal muscles that milk blood proximally back to heart • 2- pressure from breathing (inspiration decrease thoracic pressure & increase abdominal pressure • 3- intraluminal valves; unidirectional flow, open towards heart.
- In legs called “calf pump” or “peripheral pump”. • - Venous structure differs from arterial structure, walls thinner, have valves, large diameter, more distensible that expand & hold blood when blood volume increases (compensatory mechanism), this ability to stretch called capacitance vessels. • - Efficient venous return is dependent on contracting muscles, competent valves& patent lumen. Problems lead to venous stasis, risk for venous diseases are:
Who undergoes prolonged standing, sitting, or bed-rest • Hypercoagulable states • Veins trauma • Genetic predisposition • Obesity& pregnancy • Dilated & tortuous veins (varicose)
- Lymphatics: • a completely separated vessel system retrieves excess fluid from tissue spaces & returns it to bloodstream, without its drainage fluid would build up in interstitial spaces & produces edema. • Vessels drain into 2 main trunks, which empty into venous system at subclavian veins:
1) Rt lymphatic duct: empties into Rt subclavian vein, drain the Rt side of head& neck, arm, thorax, lung, heart, liver. 2) Thoracic duct: drains the rest of body, empty into Lt subclavian vein. - Functions of lymphatic system: 1- conserve fluid & plasma proteins that leak out from capillaries. 2- part of immune system( by phagocytosis & production of antibodies). 3- absorb lipids from intestinal tract.
Lymph flow is slow, propelled by contracting muscles& by pressure of breathing & by contracting of vessels itself. • Lymph nodes are small oval clumps of lymphatic tissue arranged in groups, deep & superficial (when exposed to microorganisms a local inflammation occurs & its swollen & tender). {Cervical nodes- axillary nodes- epitrochlear node- inguinal nodes}.
- Related Organs: • spleen- tonsils- thymus aid lymphatic system. • Spleen has functions: 1- destroys RBC 2- store RBC 3- filter microorganisms from blood. • Tonsilsrespond to local inflammation. • Thymus a gland in superior mediastinum behind sternum, large in fetus & children then atrophied at puberty – develop T- lymphocytes.
** Subjective Data: 1) Leg pain or cramps • 2) Skin changes on arms or legs • 3) Swelling • 4) Lymph nodes enlargement • 5) Medication
** Objective Data: • Preparations: examine arms when taking the V/S, examine legs after abdominal exam, then stand him up to evaluate leg veins, its include skin- musculoskeletal findings& neurological findings, use inspection & palpation, always compare your findings with the opposite extremity.
** INSPECT & PALPATE THE ARMS: • Lift both person’s hands in your hands, inspect, then turn them over, noting skin color & nail beds, temperature, texture, turgor, lesions, edema, clubbing, profile sign, capillary refill. Note conditions can skew your findings as a cool room; decrease body temperature, cigarette smoking, and edema. Two arms should be symmetric in size
Note scars on hands & arms, palpate both radial pulses, note rate, rhythm, elasticity of vessel wall & equal force (grades scale: +4 bounding,+3 increased, +2 normal. +1 weak, 0 absent) • Palpate the ulnar pulses • Palpate brachial pulses- both • Check epitrochlear lymph node in depression above & behind medial condyle of humerus, do this by shaking hands & reaching your other hand under person’s elbow to the groove between biceps & triceps muscles, normally not palpable.
- Modified Allen test: • evaluate the adequacy of collateral circulation prior to cannulation the radial artery, • 1- firmly occlude both ulnar & radial arteries of one hand while person makes a fist several times this cause hand to blanch • 2-ask him to open hand without hyperextending it, then release pressure on the ulnar artery while maintaining pressure on radial artery, adequate circulation is suggested by a return to normal color in 2-5 seconds.
INSPECT & PALPATE THE LEGS: • Uncover legs, inspect both legs together, noting color, hair distribution, venous pattern, size (swelling or atrophy), lesions or ulcers, note varicosities (assessed while standing), both legs should be symmetric in size, if DVT suspected, measure calf circumference at widest point, measure the other leg in exactly same place (equal), if lymphedema suspected measure also ankle, distal calf, knee& thigh, record findings.
If note ulcer or gangrene note the size & exact location. • Palpate temperature along legs down to feet, comparing symmetrically, skin should be warm, equal bilaterally, if any increase in temperature present higher up the leg, note if it is gradual or abrupt • Flex his knee; gently compress calf muscle, no tenderness. OR dorsiflex foot toward tibia, flexing knee first exerts pressure on posterior tibial vein, normally no pain.
Palpate • Homan’s Sign – calf pain with dorsiflexion (may be due to DVT) • Palpate & Grade the Pulses • Pitting Edema – Bilateral occurs w/ CHF, Diabetic neuropathy, Hepatic cirrhosis (scale of 1+ to 4+)
Palpate inguinal lymph nodes, its not unusual to find palpable nodes small, movable & non tender. • Palpate femoral, popliteal, dorsalis pedis & posterior tibial, grade the force on scale, press firmly then slowly release, Auscultate the site for a bruit
Popliteal pulse more diffuse, difficult to localize, leg extend & relaxed anchor your thumb on the knee & curl your fingers around into popliteal fossa, press fingers forward hard to compress artery against bone. If you have difficulty turn him prone & lift up lower leg, let leg relax against your arm & press in deeply with your 2 thumbs, a normal is impossible to palpate.
Posterior tibial pulse: curve fingers around medial malleolus, feel tapping in groove between malleolus & Achilles tendon, if you can’t try dorsiflextion of foot. • Dorsalis pedis pulse: very light touch, lateral & parallel with extensor tendon of big toe, over 45 years either dorsalis pedis or posterior tibial hard to find but not both of them.
Check for pretibial edema, firmly depress skin over tibia or medial malleolus for 5 second & release, normally your fingers leave no indentation, if petting edema is present, grade it on scale: • 1+ __mild pitting, slight indentation, no swelling • 2+ __ moderate pitting. Indentation subsides rapidly • 3+ __ deep pitting. Indentation remain for a short time, leg swollen • 4+ __ very deep pitting, indentation last a long time, leg very swollen
This scale subjective & qualitative, may classify by measuring depth of pitting in cm or mm or time remain after release pressure, ask person to stand so that you can assess venous system, and note any visible dilated & tortuous veins.
# Manual compression test: • person still stand-in, test length of varicose vein to determine valves competent, place one hand on the lower part of varicose vein& compress vein with your other hand about 20 cm higher, competent valves will prevent a wave transmission, distal hand will feel nothing.
# Trendelenburg test: • when varicosities present, use this test to determine valve competency. Supine position, elevate involved leg 90 degree until veins empty & place a tourniquet on thigh, help person to stand up & watch for venous filling, should be slowly in 30 seconds. After 30 seconds remove tourniquate observe whether or not the varicose veins fill suddenly from above, normally no sudden filling occurs.
# Color change: • if suspect arterial deficit, raise legs 30 cm off table ask him to wag the feet to drain off venous blood, will look a little pale but still should be pink, now let him sit up with legs over the side, compare color of both feet, note the time it takes for color to return, normally 10 seconds or less, note the time for superficial veins around feet to fill, normally 15 seconds • Blue-red color, delayed venous filling, motor & sensory loss with arterial deficits in DM
Deep Vein Thrombosis (DVT) • Deep vein occluded by:thrombus/clot • Sudden onset, pain w/dorsiflexion • Positive Homan’s sign – accurate < ⅓ of the time • Risk for PE (Pulmonary Embolism)
Aneurysm • Usually caused by atherosclerosis which weakens lining of vessel • Aorta – most common site • Effects of Blood Pressure causes ballooning of the vessel • More common in males and men over 55 & women over 70
The Aging Adult • Arteriosclerosis – blood vessel become more rigid causing a rise in systolic B/P • Atherosclerosis – Fatty plaque accumulation in the intima of arteries • Progressive enlargement of calf veins w/prolonged inactivity & heart failure leads to risk of DVT & Pulm. embolism