Download
1 / 23
620 likes | 3.88k Views
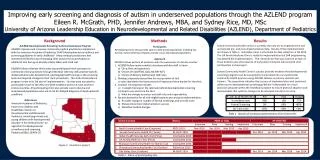
Developmental Screening. Robyn Smith Department of Physiotherapy UFS 2012. Learning objectives. Following this theme the learner must be able to: Define developmental screening Describe the screening process Define a child at risk Identify risk factors in a patient history.

E N D
Developmental Screening Robyn Smith Department of Physiotherapy UFS 2012
Learning objectives Following this theme the learner must be able to: • Define developmental screening • Describe the screening process • Define a child at risk • Identify risk factors in a patient history
Early childhood development Physiotherapists involved in early intervention services need to be knowledgeable about: • Typical development patterns • Developmental sequencing • Current developmental theories • Factors which may impact on a child’s development • Tools that can be used to screen a child in order to determine their developmental status
Developmental Screening • Screening is a brief assessment procedure designed to see whether a child's development is similar to other children of the same age • screening helps identify children who should receive a more comprehensive neurodevelopmental assessment
What is the value of developmental screening • Identifies children need comprehensive interdisciplinary assessment • Identifies children who need regular monitoring • Identify, at the earliest possible time, the presence of any developmental delays and indications of possible future disability. • Ensures the earliest possible intervention and support to infants and their families with developmental difficulties
So how do these at risk children find their way to physiotherapy services? • Routine screening of infants in neonatal unit by physiotherapist • Routine follow up of at risk infants • Referral from paediatrician • Concerned parents who bring the child to our services
Assessment procedure Parent who are concerned child is not reaching their milestones Birth Discharge Follow up More formal assessment at discharge Developmental surveillance Observation & identification risk factors Term assessment Hands off approach
A good assessment is essential in determining the cause and extent of the problem ! Only then can one discuss the implications with a parent
What does screening include? • An in-depth interview with the parent other healthcare professionals and the patient file may help identify possible risks factors
Birth History • Date of birth • Age/corrected age at present • Gestation • Birth weight • Apgar Scores • Type of delivery • Neonatal management
Identify potential risk factorsThe following medical conditions should be noted as red flag • Birth asphyxia • Very low birth weight • Premature infants • Metabolic disorders • Convulsions/seizures and epileptic syndromes • IVH & PVL • Meningitis • Congenital neurological abnormalities and genetic disorders e.g. Down Syndrome • Dimorphism • Congenital infections: • Congenital rubella • CMV • Toxoplasmosis • HIV • Arthrogryposis multiplex congenita • Maternal substance abuse • HIV-exposed
Try and identify possible intrinsic factors which may impact in development • Physiology • Anatomy • Genetics • Personality/motivation • Race/ethnicity • Medical conditions Often cannot avoid internal factors
Try and identify possible extrinsic factors which may impact in development • Inadequate bonding or nurturing with mother/caregiver • Opportunities to learn or practice • Culture • Environmental risks • Parental and child-rearing practices • Nutrition • Socio-economic factors • Trauma Often factors that can be avoided or altered
Developmental history to date • Milestones reached to date • Time frames on reaching key milestones • Any regression milestones • Immunisation status • Development in comparison to sibling • Any other developmental concerns
Objective evaluation • The second part of the screening procedure requires a more objective look at the child’s developmental abilities and lack of ability in some cases • Preferably use a valid reliable objective screening tool that covers all areas of development • Bayley Scales of Infant Development (BSID-III) • START (not quantifiable)
Physically examination Functional abilities for age & growth for age need be examined for his corrected age • Assess milestones and functional abilities for age in all areas ICF : impairment, activity and participation limitations need to be indentified • Growth charts to be plotted or use the road to health chart of the child • Normal variance of 1-2 months on either side of the expected norms
Neurological assessment • Muscle tone- active and passive • Observe for the presence of pathological reflexes
High risk infant /child Discharge once child not longer at risk of problems Developmental screening & assessment Discharge once milestones have caught up No current developmental problems Surveillance programme only Intervention & therapy and family support programme If delays are later identified intervene
How is screening programmes implemented? • Literature in favour of developmental surveillance and screening programs • Lack consensus in literature regarding implementation of such programmes. Suggested as a guideline to be followed: • 6 weeks • 3 months • 6 months • 9 months • 12 months • 18 months • 24 months annually then until school going age
What do I do with a child who I have surveyed and who by the 2 years does not show any signs of developmental delay or has caught up on his milestones? • Research has shown that these “at risk” children should be followed up annually until school going age • Perceptual, intellectual and scholastic problems will only be identified as the child gets older • Coordination and balance can also only be assesed beyond age of 2 years • If no problems are identified by school going age – DISCHARGE!
References • Images courtesy of GOOGLE Images (2010) • Mayhew, A & Price, F. 2007. Motor control in developmental neurology. Poutney, T (Ed). In Physiotherapy for children. Elsevier: Edinburough pp 73-89 • Henning, P.A. Die pasgeborebaba • Veitch, H & Kriel,H. 2006. The role of the physiotherapist in the neurodevelopment of the child. A refresher course
References • E. Brown.2001. NDT course work (unpublished) • E. Brown. 2009. Early intervention: The evalution and treatment of infants with CMD. (unpublished) • Harel, S. approach to a child with neurodevelopmental Disability. Available at: http://www.scribd.com/doc/6701564/Approach-to-a-Child-With-a-Neurodevelopmental-Disablity. Retrieved on 27 August 2009 • Versaw-Barnes, D & A. Wood. The infant at risk of developmental delay in Pediatric Physical Therapy. Tecklin, J.S. (Eds) in Pediatric Physical Therapy. Lippincott, Williams & Wilkins. Baltimore pp101 -175
References • American Academy of Pediatrics. 2001. Developmental surveillance and screening. Available online at: http://aappolicy.aappublications.org/cgi/reprint/pediatrics;108/1/192.pdf • Smith, R. 2005. The prevalence of neurological sequelae in infants with moderate to severe neonatal asphyxia. MSc.dissertation (unpublished). • Mayhew, A & Price, F. 2007.Neonatal Care in Poutney, T(ed.) Physiotherapy for Children. Elsivier.Philadelphia 73-79 • Mosby’s medical dictionary