Download
1 / 1
10 likes | 107 Views
Medication Use and Rate of Hospitalizations Among Patients Who Utilize the En-Vision ScripTalk ® Prescription Label Reader Tatyana Spektor, Bruce I Gaynes OD PharmD Department of Ophthalmology, Loyola University Chicago, Stritch School of Medicine, Maywood , IL

E N D
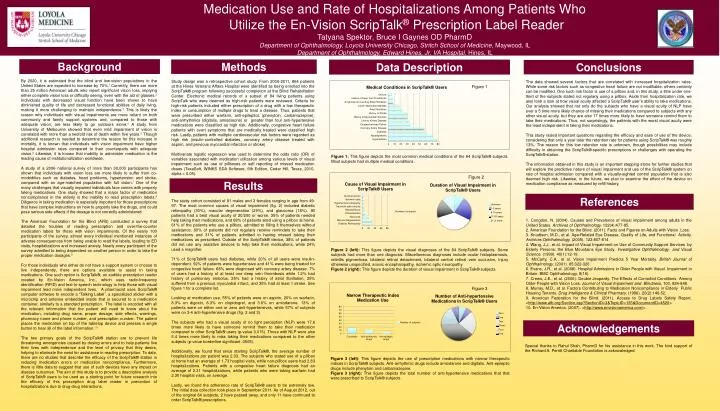
Medication Use and Rate of Hospitalizations Among Patients Who Utilize the En-Vision ScripTalk® Prescription Label Reader Tatyana Spektor, Bruce I Gaynes OD PharmD Department of Ophthalmology, Loyola University Chicago, Stritch School of Medicine, Maywood, IL Department of Ophthalmology, Edward Hines, Jr. VA Hospital, Hines, IL Background Methods Data Description Conclusions By 2020, it is estimated that the blind and low-vision populations in the United States are expected to increase by 70%.1 Currently, there are more than 25 million American adults who report significant vision loss, implying either complete vision loss or difficulty seeing, even with the aid of glasses.2 Individuals with decreased visual function have been shown to have diminished quality of life and decreased functional abilities of daily living, making it more challenging to maintain independence.3 This is likely the reason why individuals with visual impairments are more reliant on both community and family support systems and, compared to those with adequate vision, are less likely to go outdoors alone.4 A study from University of Melbourne showed that even mild impairment of vision is correlated with more than a twofold risk of death within five years.5 Though additional research is needed to determine the reason for this increase in mortality, it is known that individuals with vision impairment have higher hospital admission rates compared to their counterparts with adequate vision.6 Likewise, it is known that inability to administer medication is the leading cause of institutionalization worldwide. A study of a 2006 national survey of more than 30,000 participants has shown that individuals with vision loss are more likely to suffer from co-morbidities such as diabetes, heart problems, hypertension and stroke, compared with an age-matched population with full vision.7 One of the many challenges that visually impaired individuals face comes with properly taking medications. One study showed that a major factor of medication noncompliance in the elderly is the inability to read prescription labels.8 Diligence in taking medication is especially important for those prescriptions that have complex instructions on how to properly take the drugs, and could pose serious side effects if the dosage is not correctly administered. The American Foundation for the Blind (AFB) conducted a survey that detailed the troubles of reading prescription and over-the-counter medication labels for those with vision impairments. Of the nearly 100 participants of the survey, almost every individual mentioned instances of adverse consequences from being unable to read the labels, leading to ED visits, hospitalizations and increased anxiety. Nearly every participant of the survey admitted to being dependent on another person in order to take the proper medication dosages.9 For those individuals who either do not have a support system or choose to live independently, there are options available to assist in taking medications. One such option is ScripTalk®, an audible prescription reader created by En-Vision America, Inc., which uses radio-frequency identification (RFID) and text-to-speech technology to help those with visual impairment lead more independent lives. A pharmacist uses ScripTalk® computer software to encode a “Talking Label”, a specialized sticker with a microchip and antenna embedded inside that is secured to a medication container, similarly to a standard prescription. The label is encoded with all the relevant information that the patient will need to know about the medication, including drug name, proper dosage, side effects, warnings, pharmacy name and phone number, and prescription number. The patient places the medication on top of the tabletop device and presses a single button to hear all of the label information.10 The two primary goals of the ScripTalk® station are to prevent life threatening emergencies caused by dosing errors and to help patients live their lives with independence and the level of privacy that they desire, helping to eliminate the need for assistance in reading prescription. To date, there are no studies that describe the efficacy of the ScripTalk® station in reducing medication errors or medication noncompliance. Furthermore, there is little data to suggest that use of such devices have any impact on disease outcomes. The aim of this study is to provide a descriptive analysis of ScripTalk® users to be used as a starting point for future research into the efficacy of this prescription drug label reader in prevention of hospitalizations due to drug-drug interactions. Study design was a retrospective cohort study. From 2006-2011, 864 patients at the Hines Veterans Affairs Hospital were identified as being enrolled into the ScripTalk® program following successful completion at the Blind Rehabilitation Center. Electronic medical records of a subset of 84 living patients using ScripTalk who were deemed as high-risk patients were reviewed. Criteria for high-risk patients included either prescription of a drug with a low therapeutic index or consumption of multiple drugs to treat a disease. Thus, patients that were prescribed either warfarin, anti-epileptics (phenytoin, carbamazepine), anti-arrhythmics (digitalis, amiodarone) or greater than four anti-hypertensive medications were classified as high risk. Additionally, congestive heart failure patients with overt symptoms that are medically treated were classified high risk. Lastly, patients with multiple cardiovascular risk factors were regarded as high risk (insulin-controlled diabetes, coronary artery disease treated with aspirin, and previous myocardial infarction or stroke). Multivariate logistic regression was used to determine the odds ratio (OR) of variables associated with medication utilization among various levels of visual impairment such as use of pillboxes or self reporting of missed medication doses (TexaSoft, WINKS SDA Software, 6th Edition, Cedar Hill, Texas, 2010, alpha = 0.05). The data showed several factors that are correlated with increased hospitalization rates. While some risk factors such as congestive heart failure are not modifiable, others certainly can be modified. One such risk factor is use of a pillbox and, in this study, a little under one-third of the subjects stated not regularly using a pillbox. Aside from hospitalization rate, we also took a look at how visual acuity affected a ScripTalk® user’s ability to take medications. Our analysis showed that not only do the subjects who have a visual acuity of NLP have over a 5 time more likely chance of missing their medications compared to subjects with any other visual acuity, but they are also 17 times more likely to have someone remind them to take their medications. Thus, not surprisingly, the patients with the worst visual acuity were the least independent in taking their medications. This study raised important questions regarding the efficacy and ease of use of the device, considering that only a year later the retention rate for patients using ScripTalk® was roughly 13%. The reason for this low retention rate is unknown, though possibilities may include difficulty in obtaining the ScripTalk®-specific prescriptions or challenges with operating the ScripTalk® station. The information obtained in this study is an important stepping stone for further studies that will explore the predictive nature of visual impairment and use of the ScripTalk® system on rate of hospital admission compared with a visually-sighted control population that is also deemed high risk. Likewise, in the future, we plan to examine the effect of the device on medication compliance as measured by refill history. Figure 1 Figure 1: This figuredepicts the most common medical conditions of the 84 ScripTalk® subjects. Most subjects had multiple medical conditions. Figure 2 Results References The study cohort consisted of 81 males and 3 females ranging in age from 49-97. The most common causes of visual impairment (fig. 2) included diabetic retinopathy (30%), macular degeneration (29%), and glaucoma (18%). All patients had a best visual acuity of 20/200 or worse. 35% of patients needed help taking their medications, and 68% of patients sited using a pillbox at home. 61% of the patients who use a pillbox, admitted to filling it themselves without assistance. 80% of patients did not regularly receive reminders to take their medications and 31% of patients admitted to having missed taking their medications as prescribed. Outside of the ScripTalk® device, 38% of patients did not use any assistive devices to help take their medications, while 24% used a magnifier. 71% of ScripTalk® users had diabetes, while 20% of all users were insulin-dependent. 92% of patients were hypertensive and 41% were being treated for congestive heart failure. 68% were diagnosed with coronary artery disease. 7% of users had a history of at least one deep vein thrombosis while 1.2% had history of pulmonary embolus. 25% had a history of atrial fibrillation, 35% suffered from a previous myocardial infarct, and 35% had at least 1 stroke. See figure 1 for a complete list. Looking at medication use, 55% of patients were on aspirin, 20% on warfarin, 8.3% on digoxin, 8.3% on clopidogrel, and 3.6% on amiodarone. 13% of patients were on either one or zero anti-hypertensives, while 57% of subjects were on 3-4 anti-hypertensive drugs (fig. 2 and 3). The subjects who had a visual acuity of no light perception (NLP) were 17.6 times more likely to have someone remind them to take their medication compared to other ScripTalk® users (p-value 0.015). Those with NLP were also 5.4 times more likely to miss taking their medications compared to the other subjects (p-value borderline significant .0505). Additionally, we found that since starting ScripTalk®, the average number of hospitalizations per patient was 2.03. The subjects who stated use of a pillbox at home had an average of 1.73 hospital visits, while non-pillbox users had 2.83 hospitalizations. Patients with a congestive heart failure diagnosis had an average of 2.31 hospitalizations, while patients who were taking warfarin had 2.30 hospital visits, on average. Lastly, we found the adherence rate of ScripTalk® users to be extremely low. The initial data collection took place in September 2011. As of August 2012, out of the original 84 subjects, 2 have passed away, and only 11 have continued to order ScripTalk® prescriptions. 1. Congdon, N. (2004). Causes and Prevalence of visual impairment among adults in the United States. Archives of Ophthalmology. 122(4):477-85. 2. American Foundation for the Blind. (2011). Facts and Figures on Adults with Vision Loss. 3. Knudtson, M.D., et al. Age-Related Eye Disease, Quality of Life, and Functional Activity. Archives Ophthalmology. (2005). 123:807-814 4. Wang, J.J., et al. Impact of Visual Impairment on Use of Community Support Services by Elderly Persons: the Blue Mountains Eye Study. Investigative Ophthalmology and Visual Science. (1999). 40(1):12-19. 5. McCarty, C.A., et al. Vision Impairment Predicts 5 Year Mortality. British Journal of Ophthalmology. (2001). 85:322-326 6. Evans, J.R., et al. (2008). Hospital Admissions in Older People with Visual Impairment in Britain. BMC Ophthalmology, 8(16). 7. Crews, J.E., et al. (2006). Double Jeopardy: The Effects of Comorbid Conditions Among Older People with Vision Loss. Journal of Visual Impairment and Blindness, 100, 824-848. 8. Murray, M.D., et al. Factors Contributing to Medication Noncompliance in Elderly Public Housing Tenants. Drug Intelligence & Clinical Pharmacy. (1986). 20(2):146-52. 9. American Federation for the Blind. (2011). Access to Drug Labels Safety Report. <http://www.afb.org/Section.asp?SectionID=3&TopicID=135&DocumentID=4520>. 10. En-Vision America. (2007). <http://www.envisionamerica.com/>. Figure 2 (left): This figure depicts the visual diagnoses of the 84 ScripTalk® subjects. Some subjects had more than one diagnosis. Miscellaneous diagnoses include ocular histoplasmosis, retinitis pigmentosa, bilateral retinal detachment, bilateral central retinal vein occlusion, injury otherwise unspecified, anoxic encephalopathy, ischemic optic neuropathy Figure 2 (right): This figure depicts the duration of visual impairment in ScripTalk® subjects. Figure 3 Acknowledgements Special thanks to Rahul Shah, PharmD for his assistance in this work. The kind support of the Richard A. Perritt Charitable Foundation is acknowledged. Figure 3 (left): This figure depicts the use of prescription medications with narrow therapeutic indices in ScripTalk® subjects. Anti-arrhythmic drugs include amiodarone and digitalis. Anti-epileptic drugs include phenytoin and carbamazepine. Figure 3 (right): This figure depicts the total number of anti-hypertensive medications that that were prescribed to ScripTalk® subjects.