Download
1 / 9
90 likes | 96 Views
Blind double marking. Aim: to raise some issues contingent on the introduction of blind double marking of essay exams. BChD ( Bachelor of Dental Surgery ). 5 year course non-modular (curriculum largely determined by General Dental Council)

E N D
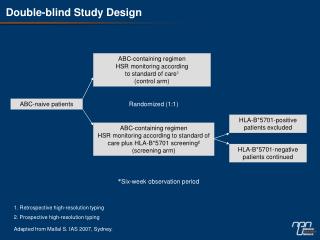
Blind double marking Aim: to raise some issues contingent on the introduction of blind double marking of essay exams
BChD (Bachelor of Dental Surgery) • 5 year course • non-modular (curriculum largely determined by General Dental Council) • degree exams in 1st, 2nd, 3rd and 5th year plus ‘Progress to Finals’
The written exam in ‘Finals’ • takes place in June of 5th year • = 40% of marks for Finals • 2 three-hour papers • 4 compulsory essay questions in each paper • each essay marked out of 25 • traditionally double-marked • first double-marked ‘blind’ in 1999
Double-marking vs.blind double-marking • traditionally 2nd marker agreed with 1st mark 70% - 80% of time and disagreements nearly always only 1 - 2 marks (out of 25) • marking blind, absolute agreement dropped to between 48% and 17% with, in one question, 35% of marks being >2 marks apart
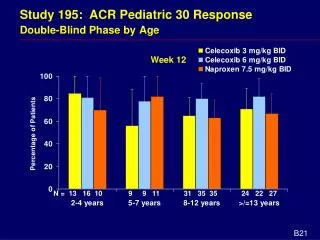
Extent of agreement between markers in 1999 final written exam
Analysis of markers’ consensus process(all questions, 48 students)
Inappropriate use of correlation statistics • Correlation statistics show association, not agreement e.g. correlation would be perfect if all marks given by 2nd marker are exactly 10 points higher than those given by 1st marker • therefore use kappa, which measures absolute agreement with reference to the frequency with which marks would be expected to agree by chance Note: agreement can be evaluated as: Poor (<0.20), Fair (0.21 - 0.40), Moderate (0.41 - 0.60), Good (0.61 - 0.80) or Very Good (0.81 - 1.00)
Standard ways of improving inter-marker reliability • re-visit assessment criteria/marking scheme • have standardisation meetings with markers • downgrade importance of essays in assessment and use more objective methods • continue to monitor marking
Action taken between June and November 1999 • Issues raised and discussed at Undergraduate Dental Education Committee and in Dental School newsletter ‘Teaching Quality Matters’ • Assessment criteria reviewed, re-formatted and published in Nathan Bodington • Markers for Operative Dentistry prize exam (December 1999) given verbal briefing about assessment criteria • Result = a marked improvement in reliability !! (but….)