Download

1 / 31
420 likes | 606 Views
Congenital megacolon. 浙江大学医学院附属儿童医院 江米足. Definition. Also called: Hirschsprung disease, HD Description: characterized by the absence of myenteric and submucosal ganglion cells in the distal intestine; usually affects the last 1-2 feet of the colon,

E N D
Congenital megacolon 浙江大学医学院附属儿童医院 江米足
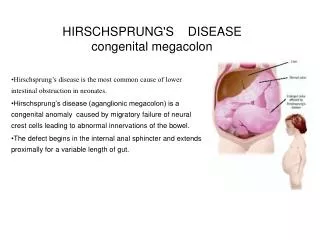
Definition • Also called: • Hirschsprung disease, HD • Description: • characterized by the absence of myenteric and submucosal ganglion cells in the distal intestine; • usually affects the last 1-2 feet of the colon, • causes problems with the movement in the affected bowel segment, • results in an obstruction of the bowel.
Organs involved • aganglionic segment always involves rectum and extends proximally without skip areas • dilated colon found proximal to aganglionic segment
Histopathology • Absence of ganglionic cells • Hypertrophic cholinergic nerve trunks • Limited number of adrenergic fiber
Who is most affected • infancy, may go undiagnosed for years • 96% are term infants, 4% are premature infants • The male to female ratio is 4:1. If the entire colon is involved, the sex ratio is about 1:1 • With an affected sibling, the incidence rises to 12-33% • occurs in 0.8% of patients with trisomy 21 Down syndrome • Incidence/Prevalence: • 1/1,000-1,500 live births
Risk factor • Risk factors for Hirschsprung's include: • Family members with the disease • More common in males • May be associated with other congenital defects
Causes and pathogenesis • Causes: • absence of submucosal and myenteric (muscular, Auerbach's) parasympathetic ganglion cells • Pathogenesis: • neuroblasts from neural crest fail to complete caudal migration to Meissner's and Auerbach's plexuses • failure of relaxation/normal peristalsis • dilatation of colon
Types 1 • aganglionic segment limited to rectosigmoid in 80% • colon aganglionic from anus to hepatic flexure in 15% (long segment HD) • entire colon lacks ganglion cells in 3% - total colonic aganglionosis, sometimes involves variable segment of distal ileum
Type 2 • Classical HD (85% of cases): Rectosegmoid • Short segment HD (10% of cases) • Long segment HD (4% of cases) • Total colonic aganglionosis (1% of cases) • rare variants include the following: • Total intestinal aganglionosis • Ultra-short-segment HD (involving the distal rectum below the pelvic floor and the anus
History • Chief concern (CC): • in infants and older children - overflow diarrhea, vomiting, abdominal distention may be enterocolitis (high mortality rate) • early symptoms of megacolon range from complete acute bowel obstruction in neonates to intermittent episodes of chronic constipation in older children
History • Chief concern (CC): • sometimes there is diarrhea, episodes of constipation and diarrhea may alternate with periods of apparent normality, diarrhea may develop into a fulminant enterocolitis leading to severe fluid and electrolyte imbalance • older children in severe cases may present with failure to thrive (FTT) and can be confused with malabsorption syndromes
History of present illness (HPI) • in infants and older children - suspect any patient with chronic unexplained illness with abnormal bowel pattern dating back to early infancy • delayed passage of meconium at birth • Past medical history (PMH): • in infants and older children - history of obstipation, constipation, failure to thrive
Physical • General physical: • in newborns - meconium ileus, intestinal obstruction, severe constipation, bilious vomiting, delayed passage of meconium (usually passed within 24 hours, 48 hours in preemies) • Abdomen: • abdominal distention, occasionally loops of stool-filled bowel palpable • Rectal: • increased sphincter tone, no stool in rectal vault, classically explosion of watery stool on removal of finger
What are the symptoms? • HD is usually diagnosed in infancy, but can also be found later. • Symptoms can differ with age
Symptoms • In newborns • Failure to pass meconium within the first 48 hours of life (Meconium is a dark sticky substance that is the first bowel movement) • Vomiting after eating • Abdominal distention • In young children • Severe constipation • Diarrhea • Anemia • Growth delay • In teenagers • Severe constipation for most of their lives • Anemia
Rule out • intestinal atresia or stenosis, congenital duodenal obstruction • imperforate anus • necrotizing enterocolitis • cystic fibrosis • malrotation • less causes of neonatal obstruction • intussusception • Meckel diverticulum • duplications • medical conditions associated with bilious vomiting and ileus • sepsis • hypothyroidism • meconium plug syndrome
“Red flags” for HD diagnosis • Delayed (>24 h) meconium—Present in 70-87% of cases of HD and in <1% of normal children • Neonatal constipation—Present in 90-95% of cases but in <7% of children with functional constipation • Family history (affected sibling)—Present in 12-33% of cases • Poor growth—Present in 25-30% of cases • Abdominal distension—Present in 76-85% of cases but in 20% of patients with functional constipation • Down’s syndrome and other chromosomal anomalies—HD is present in 1.5% of patients with Down’s syndrome, but 5-10% of patients with Down’s have functional constipation • Three or more red flags are present in 18% of patients with the disease. No red flags are present in <1% of patients with the disease
Tests for HD diagnosis • Barium enema —injection of fluid into the rectum that makes the colon show up on an x-ray • Rectal suction biopsy —removal of a sample of bowel tissue to check for ganglia, full-thickness biopsy if necessary • Anorectal manometry—measurement of the pressures of the internal and external sphincter with a rectal balloon
Imaging studies • Plain X ray: air/fluid levels, no air in rectum • Contrast enema: -Narrow distal segment -Funnel-shaped transition zone -Dilation of proximal colon -After 24-48 hours the contrast material is in the bowel -Mucosal irregularity (enterocolitis)
Abdominal x ray image • showing gaseous distension of the large bowel with air absent from the rectum (typical of HD)
Biopsy and pathology • no ganglion cells in submucosal plexus confirms diagnosis • types of rectal biopsies • seromuscular biopsy at laparotomy • full-thickness transrectal biopsy • requires bowel prep, general anesthesia • check for Auerbach's plexus • alternative - suction biopsy • small specimens, requires experienced pathologist • can be done at bedside • check for Meissner's plexus
Anorectal manometry • Normal basal internal anal sphincteric tone • No reflex relaxation of the internal sphincter with rectal distention • It can be put through safely in newborn age as well
Other diagnostic testing • Fingerprint chromatogram model of serum protein (3 protein markers) had 100% sensitivity and 100% specificity for identifying HD in 78 serum specimens (42 of HD, 16 of adhesive ileus and 20 normal controls)
Treatment • The primary treatment for HD is surgery to remove the affected portion of the colon. • There are three potential phases to the surgery, but all three phases may not be needed. • Your doctor will discuss the best methods for you or your child's condition.
Surgery • Colostomy—This involves surgically creating an opening into the colon, which is brought to the abdominal surface. Stool contents are excreted through this opening and into a bag. • Pull-through operation—The affected area of the colon is removed, then the healthy colon is brought down to the rectum and joined to the rectal wall. • Closure of the colostomy—The colostomy opening is closed, and bowel function gradually returns to normal.
Treatment Transanal Endorectal Pull-Trough • It can be performed safely in infant as well • Generally one-stage surgery • No abdominal phase • The anastomosis is happening in a “safe” place at the pectinate line
Operative sequelae • Enterocolitis rare but up to 60% mortality • Perforation of the intestine • Short gut syndrome • Anal dilation may be intermittently necessary if constipation secondary to retained aganglionic internal anal sphincter • Occasional incontinence and fecal soiling
Outcome • Symptoms are eliminated in 90% of children after surgical treatment. • A better outcome is associated with early treatment, and shorter bowel segment involvement.