Download

1 / 38
380 likes | 529 Views
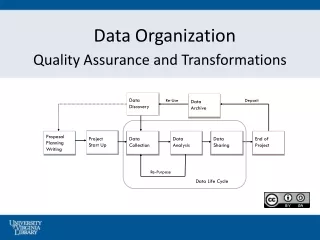
MAINE HEALTH DATA ORGANIZATION. www.mhdo.maine.gov/mhdo www.healthweb.state.me.us www.mhdpc.org. MHDO History. Established as an independent executive agency in June 30, 1996 as a result of recommendations of the Hospital Deregulation Task Force

E N D
MAINE HEALTH DATA ORGANIZATION www.mhdo.maine.gov/mhdo www.healthweb.state.me.us www.mhdpc.org
MHDO History • Established as an independent executive agency in June 30, 1996 as a result of recommendations of the Hospital Deregulation Task Force • Data collection functions of the ME Health Care Finance Commission retained, expanded and transformed into the MHDO
MHDO Established(22 MRSA §8703) • To create a useful, objective, reliable, and comprehensive health information database that is used to improve the health of Maine citizens and to issue public reports to assist consumers of health care • Governed by 20 member board representing: • 4 consumers • 3 employers • 2 third-party payers • 9 providers (2 hospital; 2 physician; 1 chiropractor; 1 pharmacist; 1 ambulatory care; 1 home health care; 1 mental health) • 2 Department of Health and Human Services (1 BMS; 1 BOH)
Powers/Duties of Board(22 MRSA §8704) • Establish uniform data systems / sets • May contract for data processing services or any other service proper or necessary • Promulgate rules to implement provisions of statutes • Hold public hearings • Hire staff • Produce annual reports • Solicit / receive grants • Cooperate with DHHS, DOL, MQF, other state agencies on various health related initiatives / research projects
Enforcement(22 MRSA §8705-A / Chapter 100) • Provides for rules to set schedule of fines for failure to submit data, failure to pay assessments, failure to safeguard identity of patients (all civil violations) • $1,000/day for health care facility, payer, TPA – not to exceed $25,000 • $100/day for all other health care providers – not to exceed $2,500 per occurrence • $250,000 maximum for intentional misuse of data for commercial advantage, pecuniary gain, or malicious harm • MHDO Board may notify the appropriate provider or payer licensing Board of the statutory violation • MHDO Board may file complaint in Superior Court • Attorney General may seek injunctive relief against any violator
Revenues(22 MRSA §8706 /Chapter 10) • Provides authority to equally assess health care providers and payers for the total allowable revenue to be collected in the following percentages: • 38.5% hospitals (based upon net patient service revenue) • 11.5% non-hospital providers (based upon fixed categorical assessments) • 38.5% carriers (based upon premiums written) • 11.5% TPA’s (based upon claims paid for plan sponsors)
Revenues(22 MRSA §8706 / Chapter 50) • Provides authority to establish fees charged for purchasing data sets, special programming time, and other costs associated with data requests such as: duplicating, mailing, publishing, supplies • Fees may be reduced or waived for research of general benefit to public health or inability to pay
Expenditures(22 MRSA §8706) • Legislatively authorized total expenditures / assessment cap: • FY2006 - $1,627,585 • FY2007 - $1,708,964 • 9 positions; 4FTE’s @ MHDPC • Funds not expended must be carried forward to reduce following FY assessment
Data Release(22 MRSA §1711-C(1)(E) / Chapter 125) • MHDO Board required to define direct identifiers through rules as part of comprehensive health care information confidentiality legislation • Direct identifiers referenced in Chapter 120
Data Release(22 MRSA §8707 / Chapter 120) • Provides authority to establish terms and conditions of data release: • No direct (Ch. 125) / indirect identification of patients – unless MHDO Board grants exception to DHHS for public health study • Direct identification of individual practitioners currently protected • Identity of practitioners performing abortions protected • No release of data deemed confidential or privileged (discounts, capitation) by MHDO – data providers may challenge designation • No release of data that places data provider at a competitive economic disadvantage • Data providers may review all data requests, require additional information, and/or require further review prior to data release
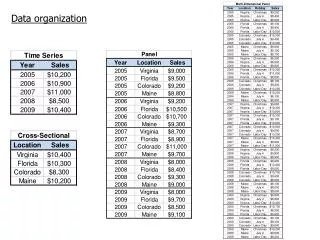
MHDO Databases • Hospital inpatient • Hospital outpatient • Hospital emergency department • Non-hospital ambulatory services • All provider/all payer health care claims • Quality data • Hospital financial and organizational
MHDO Databases (continued) • Available Data Elements: • Patient demographics (date of birth, age, gender, town state, zip code, encrypted ssn) • Provider identification (name of facilities, specialty codes, encrypted practitioner codes) • Diagnosis (including E-codes)/procedure codes • Procedure/service dates • Payer identification • Charges/payments (including co-pay, coinsurance, deductibles)
Hospital Data(22 MRSA §8708 / Chapter 241) • 39 Maine non-federal hospitals required to submit inpatient and outpatient records for all encounters • Submitted for each geographically separated facility via AmeriNet Central Patient Data Check in-hospital editing system • Based upon UB-92 billing and medical records data • MHDO may require additional medical abstract data
Hospital Data (continued)(22 MRSA §8708 / Chapter 241) • Inpatient: • Initiated 1978, data available from 1980 • Approximately 160,000 patient level records/year • Outpatient: • Initiated 1996, data available from 1998 • Only complete hospital outpatient database in US • Approximately 1,400,000 visit level records/year • Over 8,000,000 detail records/year • Emergency Department: • Created from inpatient/outpatient data • Data available from January, 2003 • Approximately 72,000 inpatient and 574,000 outpatient records/year
Claims Data(22 MRSA §8708 / Chapter 243) • Data submitted by approximately 150 Maine licensed health insurance carriers and third-party administrators for covered Maine residents • MaineCare and Medicare data to be included in 2005 • Does not include uninsured and claims related to disability, long-term care, or specialty policies • Comprised of four files – eligibility, medical, pharmacy, dental • Approximately 50,000,000 records/year • Data available from January, 2003 • Eighteen months of data available March of 2005
Claims Data (continued)(10 MRSA Ch. 102-A) • ME Health Data Processing Center established June 28, 2001 • Public/private partnership – MHDO/MHIC: 60%/40% funding • Center receives and processes claims data in accordance with Ch. 243 • All data stored at and released by MHDO
Ambulatory Services Data(22 MRSA §8708 / Chapter 245) • 70 licensed non-hospital providers required to submit data related to specific procedures (not entire patient population) • Data available from 1990 • Approximately 50,000 records/year • Database to be eliminated in March, 2005 due to incomplete / inaccurate data and the creation of the claims database
Quality Data(22 MRSA §8708-A 7 / Chapter 270) • Authority provided to collect data based upon measures adopted by the ME Quality Forum • Initial quality data sets include: • Twenty nine quality measures from 39 hospitals • Three quality measures from 18 ambulatory surgical centers
Financial Data(22 MRSA §8709 / Chapter 300) • Authority provided to collect financial information and scope of service data (bed capacity, special services, clinical specialties) from all health care facilities • Currently only audited financial statements with supplemental information regarding discount rates and Medicare Cost Reports collected from 39 hospitals • Standardized annual hospital financial summaries proposed for 2005 • Information available from 2000
Restructuring Data(22 MRSA §8710 / Chapter 630) • Authority provided to require all providers and payers to submit occurrence of major structural changes to the delivery and financing of health care • Currently only required from hospitals and parent organizations • Submissions incomplete and compliance marginal
Other Data(22 MRSA §8711) • Authority to require all providers and payers to submit additional information in order to modify data collection systems • Pilot information systems may also be required
Mandatory Annual Reports(22 MRSA §8712) • Quality – in conjunction with MQF • Price – prices paid for fifteen most common services provided by facilities and practitioners • Comparison – fifteen most common hospital inpatient / outpatient procedures and non-hospital procedures compared to similar data in other states • Physician services – ten most often provided services / procedures in office setting
Overview of Maine Health Care Claims Database • Legislation passed in June of 2001 creating the Maine Health Data Processing Center (a public/private partnership between the Maine Health Data Organization and the Maine Health Information Center) • Additional legislation passed in 2001 to expand the data collection authority of the MHDO to include Third-Party Administrators • Health care claims data collection rules finalized in July of 2002
Overview (continued) • System for receiving / editing the data constructed between August and December, 2002 • Data submissions begin in January, 2003 • First iteration of data to be released in March of 2005 • Operational costs of MHDPC – approximately $450,000 / year (will stabilize or drop in two years)
Overview (continued) • Database contains: • Paid medical, dental, pharmacy claims files for services rendered to commercially insured, and Medicare and MaineCare covered Maine residents • Eligibility/membership files • Health care provider files • Data submitted by payers (based upon # of members): • Monthly (>2,000) • Quarterly (500-1,999) • Annually (<500s) • Standard format utilized: • HIPAA standard codes • HIPAA transaction set data elements (ASC X12N 270/271 eligibility, 835 remittance, 837 claims)
Overview (continued) • Information not presently included in the database: • Services provided to uninsured • Denied claims • Workers’ compensation claims • Services by Maine providers for non-Maine residents • Premium information • Capitation fees • Administrative fees • Referrals • Test results from lab work, imaging, etc. • Prescribing physician • Provider affiliation with group practice • Provider networks
Overview (continued) • Information included in the database: • Encrypted social security numbers • Type of product (HMO, POS, Indemnity, etc.) • Type of contract (single person, family, etc.) • Patient demographics (date of birth, gender, residence, relationship to subscriber) • Diagnosis codes (including E-codes) • Procedure codes (ICD, CPT, HCPC, CDT) • NDC code / generic indicator • Revenue codes
Overview (continued) • Information included in the database (continued): • Revenue codes • Service dates • Service provider (name, tax id, payer id, specialty code, city, state, zip code) • Plan payments • Member payment responsibility (co-pay, coinsurance, deductible) • Date paid • Type of bill • Facility type
Status of Claims Database( January 2003 – September 2004): • Data submitted from 150 of mandated commercial carriers / TPA’s • Claims data (30 GB): • 28 million medical records • 12 million pharmacy records • 3 million dental records • Eligibility data (11 GB) - one record / eligible member / month: • 19 million medical member records • 13 million pharmacy member records • 9 million dental member records
Issues / Problems • #1 - Enactment of Health Insurance Portability and Accountability Act of 1996 (HIPAA) with associated ASC X12N standards will bring uniformity to the health care claims process. • Reality: • Payers do not retain data for all fields submitted by providers in their data warehouses (not needed to pay claims) • Providers do not submit data for all required fields (not needed to pay claims so not enforced by payers) • Most providers and payers do not use required adopted national specialty code taxonomy • Home grown diagnosis codes still germinate and thrive • 15-20% of claims still submitted in paper resulting in missing data
Issues / Problems • Reality (continued): • National patient ID does not exist – have resorted to using encrypted SSN’s for subscribers/members (exist for 90% of ME residents but movement nationally to eliminate use in health related databases) • National payer ID not yet established (difficult to track mergers, buy outs, DBA’s) • National provider ID delay has resulted in additional complexities and expenses ($100,000+) in order to: • Strip provider information out of the claims and create a provider file • Standardize provider specialty coding using national specialty taxonomy codes • Add other data sources (State Boards of Licensure, published network information) • Link data using all possible data points and conduct manual review
Issues / Problems • #2: - Adding Maine’s patient level Medicaid data to the claims database will be beneficial to the Medicaid program (utilization/price comparisons, dual eligibility evaluation, etc.) and will occur through an MOA. • Reality: Some Maine Medicaid administrators, Region I CMS staff, and subsequently CMS Headquarters have impeded/prevented the data transfer providing ambiguous and archaic legal arguments.
Issues / Problems • #3 - It will be next to impossible to obtain the patient level Medicare data for ME residents and incorporate it into the claims database for re-release. • Reality: MHDO’s request for patient level data was granted by CMS headquarters on October 15, 2004 (incorporation occurring over the next three months).
Issues / Problems • #4 - The Employer Retirement Income Security of 1974 (ERISA) will preempt the MHDO from securing claims data from third-party administrators acting on behalf of plan sponsors. • Reality: On March 24, 2004 U.S. District Court Judge J. Brock Hornby ruled that health care claims data held by a TPA are not a plan asset and, consequently, must be provided to the MHDO under Maine law.
Projected Uses of Claims Database • Determine utilization patterns and rates for Maine residents (including procedures by geographical area, trends over time, cost per member per month for services by provider and population group, population‑based rates of services) • Identification of gaps in needed disease prevention and health promotion services • Evaluate access to care (including ER use by area, severity of cases by primary care doctors vs. specialists, preventive services by population group) • Assist with benefit design and planning for Maine's newly established governmental health insurance program (Dirigo Health) to cover the uninsured population
Projected Uses (continued) • Analyze statewide health care expenditures (including paid data comparisons for types of services, combined treatment, Rx vs. medical costs, etc.) • Establish clinical guideline measurements related to quality, safety, and continuity of care • Analyze the Medicare / MaineCare (Medicaid) dual eligibility population
Expense Per Member Per Month (PMPM)Members with Medical and Pharmacy Commercial Coverage and Continuous Enrollment