Download
1 / 1
10 likes | 76 Views
Looks Gassy: Pneumobilia Status Post Hydrogen Peroxide Ingestion. Vamsi Balakarishna, MD, Regina Hart, DO, Jennifer Axelband, DO St. Luke’s University Health Network. Introduction. Case Report 2. Discussion.

E N D
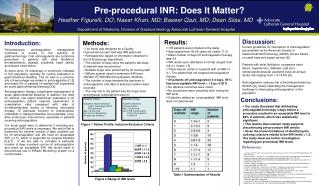
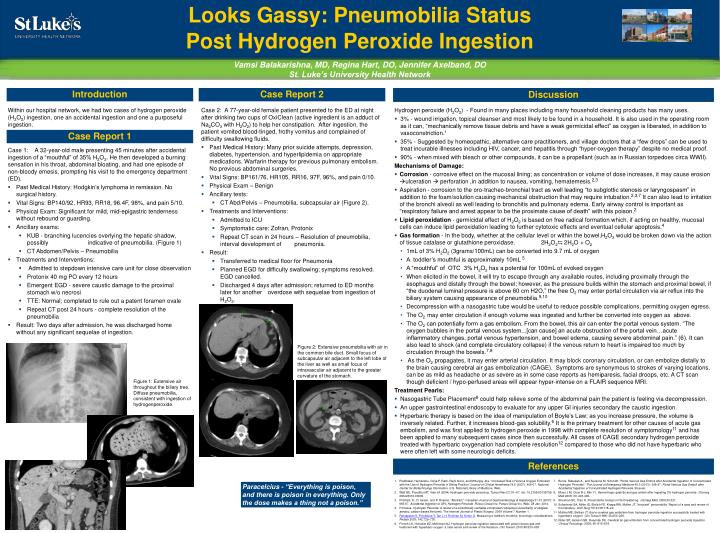
Looks Gassy: Pneumobilia Status Post Hydrogen Peroxide Ingestion Vamsi Balakarishna, MD, Regina Hart, DO, Jennifer Axelband, DO St. Luke’s University Health Network Introduction Case Report 2 Discussion Within our hospital network, we had two cases of hydrogen peroxide (H2O2) ingestion, one an accidental ingestion and one a purposeful ingestion. • Case 2: A 77-year-old female patient presented to the ED at night after drinking two cups of OxiClean (active ingredient is an adduct of Na2CO3 with H2O2) to help her constipation. After ingestion, the patient vomited blood-tinged, frothy vomitus and complained of difficulty swallowing fluids. • Past Medical History: Many prior suicide attempts, depression, diabetes, hypertension, and hyperlipidemia on appropriate medications. Warfarin therapy for previous pulmonary embolism. No previous abdominal surgeries. • Vital Signs: BP161/76, HR105, RR16, 97F, 96%, and pain 0/10. • Physical Exam – Benign • Ancillary tests: • CT Abd/Pelvis – Pneumobilia, subcapsular air (Figure 2). • Treatments and Interventions: • Admitted to ICU • Symptomatic care: Zofran, Protonix • Repeat CT scan in 24 hours – Resolution of pneumobilia, interval development of pneumonia. • Result: • Transferred to medical floor for Pneumonia • Planned EGD for difficulty swallowing; symptoms resolved. EGD cancelled. • Discharged 4 days after admission; returned to ED months later for another overdose with sequelae from ingestion of H2O2. • Hydrogen peroxide (H2O2) - Found in many places including many household cleaning products has many uses. • 3% - wound irrigation, topical cleanser and most likely to be found in a household. It is also used in the operating room as it can, “mechanically remove tissue debris and have a weak germicidal effect” as oxygen is liberated, in addition to vasoconstriction.1 • 35% - Suggested by homeopathic, alternative care practitioners, and village doctors that a “few drops” can be used to treat incurable illnesses including HIV, cancer, and hepatitis through “hyper-oxygen therapy” despite no medical proof. • 90% - when mixed with bleach or other compounds, it can be a propellant (such as in Russian torpedoes circa WWII). • Mechanisms of Damage: • Corrosion - corrosive effect on the mucosal lining; as concentration or volume of dose increases, it may cause erosion ulceration perforation ,in addition to nausea, vomiting, hematemesis.2,3 • Aspiration - corrosion to the oro-tracheo-bronchial tract as well leading “to subglottic stenosis or laryngospasm” in addition to the foam/solution causing mechanical obstruction that may require intubation.2,3,7 It can also lead to irritation of the bronchi alveoli as well leading to bronchitis and pulmonary edema. Early airway control is important as “respiratory failure and arrest appear to be the proximate cause of death” with this poison.2 • Lipid peroxidation - germicidal effect of H2O2 is based on free radical formation which, if acting on healthy, mucosal cells can induce lipid peroxidation leading to further cytotoxic effects and eventual cellular apoptosis.4 • Gas formation - In the body, whether at the cellular level or within the bowel,H2O2 would be broken down via the action of tissue catalase or glutathione peroxidase. 2H2O2⇆ 2H2O + O2 • 1mL of 3% H2O2 (3grams/100mL) can be converted into 9.7 mL of oxygen • A toddler’s mouthful is approximately 10mL 5 • A “mouthful” of OTC 3% H2O2 has a potential for 100mL of evoked oxygen • When elicited in the bowel, it will try to escape through any available routes, including proximally through the esophagus and distally through the bowel; however, as the pressure builds within the stomach and proximal bowel, if “the duodenal luminal pressure is above 60 cm H2O,” the free O2 may enter portal circulation via air reflux into the biliary system causing appearance of pneumobilia.9,10 • Decompression with a nasogastric tube would be useful to reduce possible complications, permitting oxygen egress. • The O2 may enter circulation if enough volume was ingested and further be converted into oxygen as above. • The O2 can potentially form a gas embolism. From the bowel, this air can enter the portal venous system. “The oxygen bubbles in the portal venous system...[can cause] an acute obstruction of the portal vein…acute inflammatory changes, portal venous hypertension, and bowel edema, causing severe abdominal pain.” (6). It can also lead to shock (and complete circulatory collapse) if the venous return to heart is impaired too much by circulation through the bowels.7,8 • As the O2 propagates, it may enter arterial circulation. It may block coronary circulation, or can embolize distally to the brain causing cerebral air gas embolization (CAGE). Symptoms are synonymous to strokes of varying locations, can be as mild as headache or as severe as in some case reports as hemiparesis, facial droops, etc. A CT scan though deficient / hypo-perfused areas will appear hyper-intense on a FLAIR sequence MRI. • Treatment Pearls: • Nasogastric Tube Placement8 could help relieve some of the abdominal pain the patient is feeling via decompression. • An upper gastrointestinal endoscopy to evaluate for any upper GI injuries secondary the caustic ingestion. • Hyperbaric therapy is based on the idea of manipulation of Boyle’s Law; as you increase pressure, the volume is inversely related. Further, it increases blood-gas solubility.6 It is the primary treatment for other causes of acute gas embolism, and was first applied to hydrogen peroxide in 1998 with complete resolution of symptomology11 and has been applied to many subsequent cases since then successfully. All cases of CAGE secondary hydrogen peroxide treated with hyperbaric oxygenation had complete resolution12 compared to those who did not have hyperbaric who were often left with some neurologic deficits. Case Report 1 Case 1: A 32-year-old male presenting 45 minutes after accidental ingestion of a “mouthful” of 35% H2O2. He then developed a burning sensation in his throat, abdominal bloating, and had one episode of non-bloody emesis, prompting his visit to the emergency department (ED). • Past Medical History: Hodgkin’s lymphoma in remission. No surgical history. • Vital Signs: BP140/92, HR93, RR18, 96.4F, 98%, and pain 5/10. • Physical Exam: Significant for mild, mid-epigastric tenderness without rebound or guarding. • Ancillary exams: • KUB - branching lucencies overlying the hepatic shadow, possibly indicative of pneumobilia. (Figure 1) • CT Abdomen/Pelvis – Pneumobilia • Treatments and Interventions: • Admitted to stepdown intensive care unit for close observation • Protonix 40 mg PO every 12 hours • Emergent EGD - severe caustic damage to the proximal stomach w/o necrosi • TTE: Normal; completed to rule out a patent foramen ovale • Repeat CT post 24 hours - complete resolution of the pneumobilia • Result: Two days after admission, he was discharged home without any significant sequelae of ingestion. Figure 2: Extensive pneumobilia with air in the common bile duct. Small focus of subcapsular air adjacent to the left lobe of the liver as well as small focus of intravascular air adjacent to the greater curvature of the stomach. Figure 1: Extensive air throughout the biliary tree. Diffuse pneumobilia, consistent with ingestion of hydrogenperoxide. References Prabhakar, Hemanshu, Girija P. Rath, RajniArora, and MritunjayJha. "Increased Risk of Venous Oxygen Embolism with the Use of Hydrogen Peroxide in Sitting Position."Journal of Clinical Anesthesia 19.5 (2007): 406-07. National Center for Biotechnology Information. U.S. National Library of Medicine. Web. Watt BE, Proudfoot AT, Vale JA (2004) Hydrogen peroxide poisoning. Toxicol Rev 23: 51–57. doi: 10.2165/00139709-200423010-00006 Pritchett, S., D. Green, and P. Rossos. "Abstract." Canadian Journal of Gastroenterology & Hepatology 21.10 (2007): 665-67. Accidental Ingestion of 35% Hydrogen Peroxide, Pulsus Group Inc. Pulsus Group Inc. Web. 28 Jan. 2014. R Howes. Hydrogen Peroxide: A review of a scientifically verifiable omnipresent ubiquitous essentiality of obligate, aerobic, carbon-based life forms. The Internet Journal of Plastic Surgery. 2009 Volume 7 Number 1. Ratnapalan S, Potylitsina Y, Tan L H, Roifman M, Koren G. Measuring a toddler's mouthful: toxicologic considerations.Pediatr 2003; 142:729–730. French LK, Horowitz BZ, McKeown NJ. Hydrogen peroxide ingestion associated with portal venous gas and treatment with hyperbaric oxygen: a case series and review of the literature. ClinToxicol. 2010;48:533–538 Burns, Rebekah A., and Suzanne M. Schmidt. "Portal Venous Gas Emboli after Accidental Ingestion of Concentrated Hydrogen Peroxide." The Journal of Emergency Medicine 45.3 (2013): 346-47. Portal Venous Gas Emboli after Accidental Ingestion of Concentrated Hydrogen Peroxide. Elsevier. Moon J M, Chun B J, Min Y I. Hemorrhagic gastritis and gas emboli after ingesting 3% hydrogen peroxide. J Emerg Med 2006; 30: 403-406. Sherman SC, Tran H. Pneumobilia: benign or life-threatening. J Emerg Med. 2006;30:221. Schechner SA, Miller ID, Ehrlich FE, Knapp RW, Mullen JT. “Innocent” pneumobilia. Report of a case and review of the literature. Arch Surg 1974;108:118–20. Mullins ME, Beltran JT. Acute cerebral gas embolism from hydrogen peroxide ingestion successfully treated with hyperbaric oxygen. ClinToxicol 1998; 36:253–256. Rider SP, Jackson SB, Rusyniak DE. Cerebral air gas embolism from concentrated hydrogen peroxide ingestion. Clinical Toxicology. 2008; 46: 815–818. Paracelcius - “Everything is poison, and there is poison in everything. Only the dose makes a thing not a poison.”