Download
1 / 40
400 likes | 535 Views
The European Group for Blood and Marrow Transplantation. STEM CELL TRANSPLANTATION FOR PATIENTS WITH WALDENSTROM’S MACROGLOBULINEMIA (WM) Dr Charalampia Kyriakou MD, PhD. WALDENSTROM’S MACROGLOBULINEMIA. Rare Indolent Lymphoma

E N D
The European Group for Blood and Marrow Transplantation STEM CELL TRANSPLANTATION FOR PATIENTS WITH WALDENSTROM’S MACROGLOBULINEMIA (WM) Dr Charalampia Kyriakou MD, PhD
WALDENSTROM’S MACROGLOBULINEMIA • Rare • Indolent Lymphoma • Median presentation age 63 years-often have ongoing morbidities from other diseases • Smoldering - Asymptomatic WM - NO TREATMENT • Conventional Therapies up to 90% response, short duration and low CR rates • No cure
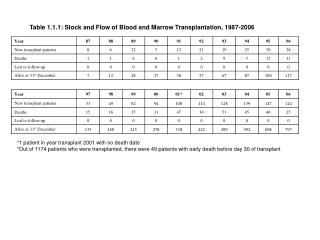
WALDENSTROM’S MACROGLOBULINEMIAISSWM Adverse covariates: .Age>65 . Hb≤11.5g/dL .Plt≤100x109/L .IgM>70g/L .Β2-M>3mg/L ?LDH ?CRP ?Previous Line therapies Risk Score * No of pts (%) {n=587 Median FU 5.3yrs} 5yrs survival (%) Low ≤1, Age<65 155(27) 87 Intermediate 2 or Age>65 224(38) 68 High >2 208(35) 36 Risk- LDH-Previous Rx Lines ** No of pts (%) {n=183 Median FU 10yrs} 8yrs survival(%) Low - Normal LDH 98 55 Low-Intermediate – High LDH 51 33 High - Normal LDH 29 5 High - High LDH 4 0 *Morel et al; Blood 113:4163-4170, 2009 **Dhodapkar et al; Blood 113:793-796,2009
STEM CELL TRANSPLANTATION FOR WM PATIENTS • Anagnostopoulos et al Biol Blood Marrow Transplant. Aug;2006 • Tournilhac et al Semin Oncol. Apr;2003 • P. Dreger, N. Schmitz Biol Blood Marrow Transplant. May;2007 • David Maloney; IWMW;Venice, Italy ,2010
Haematopoietic Stem Cell Transplantation Objectives • Deliver high - lethal dose chemo-radio therapy to destroy tumour cells • Provide a source of haemopoietic stem cells to salvage the ablated marrow • Establish organ graft tolerance to prevent rejection of donor cells • Provide immune effector cells to mediate graft-vs-tumour activity E.D. Thomas et al, N. Engl. J. Med. 257, 491-496 (1957) Intravenous Infusion of Bone Marrow in Patients Receiving Radiation and Chemotherapy
Autologous/Allogeneic Stem Cell Transplantation • Cells either obtained from G-CSF/+ Chemotherapy (for ASCT) mobilised peripheral blood stem cells or bone marrow harvest • Requires HLA-matched donor • Matched sibling (25% chance of matching any sibling) • Umbilical cord blood cells • Mismatched donors • Matched unrelated donor • Search International donor registries
Cy / TBI By/TBI Melp/VP16/TBI Cyclo/VP16/BCNU Flu / Mel / Campath Flu / Bu / ATG Flu / TBI 2Gy Immunosuppressive Flu / Cy BEAM Campath TBI 2Gy FLAG / Ida Myelosuppression Regimen Intensity for Allogeneic Stem Cell Transplantation Conventional Myeloblative Reduced Intensity
Low toxicity and TRM Low incidence of GVHD High level of tumour control Good immune reconstitution Disease responds to DLI The Perfect Transplant Regimen
Sources of Stem Cell Transplantation • Allogeneic • Stem cells free of WM • Undamaged stem cells • Immune mediated graft-vs-tumour effect • Replaces damaged host haemopoiesis • DLI may provide augmented anti-WM activity • May be curative • More toxicity, GVHD • Lower Relapse rates • Autologous • Donor available • No GVHD • No Immunosuppression • Less toxicity • Higher relapse rates
Questions ??? • Can Stem Cell Transplantation be used as a curative approach to WM? • WHO • ?Indication • ?Risk-benefit • ?Recipient Performance Status, Specific HCT comorbidity index, risk score for mortality • WHEN • ?Not too early not too late ? “frontline” • ?Age • ?Response target? Cure ? Significance of disease status pre-post on the overall management • ?Long term risks • TYPE • ?Conditioning ?Auto ?Allo ?MAC ?RIC?Intensity?SIB?MUD • ?GVHD prophylaxis ?purging
67% 67% 25% ALLOGENEIC STEM CELL TRANSPLANTATION FOR HIGH RISK WM PATIENTS (n=25, MAC:12, RIC:13) Median FU: 64 (11-149) months , Heavily pre-treated, 44% chemorefractory Dx Garnier et al, Haematologica 2010
Allogeneic Stem Cell Transplantation For High Risk WM Patients (n=25) Garnier et al, Haematologica 2010
Allo-SCT Auto-SCT EBMT Lymphoma Registry WM-SCT Activity1995-2007 SCT activity by year of SCT
WM ASCT – RESULTS (n=158) • Median Follow-up for the surviving pts, years (range): 4.2 (0.5- 14.8) • Alive: n= 107 (68%) • No progression: n=78 (49%) • Relapse or progression: n=71(45%) • Time to relapse or progression: 15m (1-110) • Dead: 51 (32%) • Disease progression: 42 (26%) • Non-disease Progression: 9 (8%) Infection:6, MOF:2, Cardiac:1 Secondary Malignancies: 10 (6.3%) [AML: 1, MDS: 4, Melanoma: 1,Prostate Ca: 1, Small Cell Lung Ca: 1, Other solid tumors: 2] Kyriakou et al, JCO 2010
Post- Autologous Stem Cell Transplantation (ASCT) Outcome by disease status at the time of ASCT (n=158) Kyriakou et al, JCO 2010
1.0 0.5 0.8 0.4 Relapse or Progression 52% 0.6 0.3 Secondary malignancies Cumulative Inidenece Cum Inc Sec Malignancy 0.2 0.4 8.4% NRM 0.1 0.2 5.6% 4.6% 3.8% 0.0 0 2 4 6 8 10 0.0 Time after ASCT (years) 0 1 2 3 4 5 6 7 8 Time after ASCT (years) Non Relapse Mortality – Relapse Rate - ASCT Kyriakou et al, JCO 2010
OS:VGPR1, PR1 1.0 OS: ALL PTS 1.0 84% 77.6% 77% 68.5% 0.8 0.8 73% 0.6 0.6 61.7% PFS: VGPR1, PR1 Probability of Survival Probability of Survival 52% PFS: ALL PTS 0.4 0.4 41% 0.2 0.2 0.0 0.0 0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8 Time after ASCT (years) Time after ASCT (years) Progression Free And Overall Survival - ASCT Kyriakou et al, JCO 2010
Progression Free And Overall Survival By Immunofixation 1.0 n.s. - IF (n=33) 1.0 p=0.08 0.8 0.8 0.6 - IF (n=33) 0.6 + IF (n=18) Overall Survival PFS 0.4 0.4 + IF (n=18) 0.2 0.2 Landmark: 6 months Landmark: 6 months 0.0 0.0 0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8 Time after ASCT (years) Time after ASCT (years) Kyriakou et al, JCO 2010
Adverse prognostic Factors for Post ASCT Outcome: Multivariate analysis Kyriakou et al, JCO 2010
Progression Free and Overall Survival By disease Status at ASCT 1.0 1.0 Chemosensitive disease 0.8 Chemosensitive 0.8 0.6 0.6 PROGRESSION FREE SURVIVAL p<0.001 p<0.001 OVERALL SURVIVAL 0.4 0.4 Chemorefractory disease 0.2 0.2 Chemorefractory 0.0 0.0 0 12 24 36 48 60 72 0 12 24 36 48 60 72 Months after ASCT Months after ASCT
100% 75% MAC 50% RIC 25% 0% 2000 2001 2002 2003 2004 2005 2006 2007 EBMT Lymphoma Registry: Allo-SCT-WM: 2000-2007 (n=86; MAC:37, RIC:49 pts) Allo-SCT: Conditioning by year of SCT 32% Chemo-refractory disease, 47% High and 19% Intermediate risk Dx, 10% poor performance status
WM Allo-SCT - Results Kyriakou et al; JCO 2010
WM Allo-SCT - Results – Donor Lymphocyte Infusion Kyriakou et al; JCO 2010
Results Post Allo-SCT - GVHD Kyriakou et al; JCO 2010
Impact Of Chronic - GVHD On Relapse Rate And Progression Free Survival 1.0 1.0 cGVHD (n=21) 0.8 0.8 p=0.03 0.6 p=0.1 0.6 No cGVHD (n=31) RELAPSE OR PROGRESSION PROGRESSION FREE SURVIVAL 0.4 0.4 No cGVHD (n=31) 0.2 0.2 cGVHD (n=21) 6 mo 6 mo 0.0 0.0 0 1 2 3 4 5 6 0 1 2 3 4 5 6 Years after Allo-SCT Years after Allo-SCT Kyriakou et al; JCO 2010
WM Allo-SCT Non - Relapse Mortality (n=86) 1.0 1.0 0.8 0.8 Whole series (n=86) 0.6 0.6 NRM NRM p: n.s. MAC (n=37) 0.4 0.4 27% 23% 0.2 0.2 RIC (n=49) 0.0 0.0 0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8 Years after Allo-SCT Years after Allo-SCT Kyriakou et al; JCO 2010
WM Allo-SCT Relapse / Progression (n=86) 1.0 1.0 0.8 0.8 p: n.s. 0.6 0.6 Whole series (n=86) RELAPSE OR PROGRESSION RELAPSE OR PROGRESSION 0.4 RIC (n=49) 0.4 19% 15% MAC (n=37) 0.2 0.2 0.0 0.0 0 1 2 3 4 5 6 7 8 0 1 2 3 4 5 6 7 8 Years after Allo-SCT Years after Allo-SCT Kyriakou et al; JCO 2010
WM Allo-SCT Overall and Progression Free Survival 1.0 1.0 Whole series (n=86) Whole series (n=86) 72% 0.8 0.8 61% 66% 64% 52% 0.6 0.6 PROGRESSION FREE SURVIVAL 0.4 0.4 OVERALL SURVIVAL 0.2 0.2 0.0 0 1 2 3 4 5 6 7 8 0.0 Years after Allo-SCT 0 1 2 3 4 5 6 7 8 Years after Allo-SCT Kyriakou et al; JCO 2010
Stem cell Transplantation (ASCT vs RIC vs MAC) EBMT Database reported between Jan 2000- Jan 2010 First SCT procedure ASCT n=424 Allo SCT n=226 RIC n=139 MAC n=81 10 years experience on Stem Cell Transplantation in patients with Waldenstrom MacroglobulinemiaEBMT Update
1,00 ASCT 0,75 RIC-Allo-SCT MAC-Allo-SCT 0,50 Cumulative Incidence 0,25 0,00 0 12 24 36 48 60 72 84 Months post-SCT NRM: ASCT - RIC - MAC - Allo-SCT
ASCT 1,00 RIC-Allo-SCT 0,75 MAC-Allo-SCT Cumulative Incidence 0,50 0,25 0,00 0 12 24 36 48 60 72 84 Months post-SCT RR: ASCT - RIC – MAC - Allo-SCT
1,00 ASCT 0,75 Allo-SCT 0,50 Cumulative Survival 0,25 0,00 0 12 24 36 48 60 72 84 96 108 120 Months post-SCT PFS: ASCT – Allo - SCT p=0.001
ASCT 1,00 RIC-Allo-SCT 0,75 MAC-Allo-SCT 0,50 Cumulative survival 0,25 0,00 0 12 24 36 48 60 72 84 96 108 120 Months post-SCT PFS: ASCT - RIC - MAC - Allo- SCT
1,00 ASCT 0,75 Allo-SCT 0,50 Cumulative Survival 0,25 0,00 0 12 24 36 48 60 72 84 96 108 120 Months post-SCT OS: ASCT - Allo- SCT
1,00 ASCT RIC-Allo-SCT 0,75 MAC-Allo-SCT 0,50 Cumulative survival 0,25 0,00 0 12 24 36 48 60 72 84 96 108 120 Months post-SCT Overall Survival: ASCT - RIC – MAC - Allo- SCT
Treatment answers from Collaborative International Randomised clinical trials Patients with high risk WM have poor prognosis with conventional therapy HDT and SCT should be considered as a therapeutic option for high risk WM patients Autologous Stem Cell Transplantation Low NRM Prolonged PFS and OS. Significantly superior ASCT outcomes were observed in patients with chemosensitive disease transplanted early following 1st maximum response Note risk for secondary malignancies but comparable to the published incidence with conventional Rx Could be considered for selected younger patients with high risk disease Allogeneic –Stem Cell Transplantation High transplant related toxicity - Compromised Overall and Progression Free Survival Consider Allo-SCT only for high risk WM younger and fit patients with relapse refractory disease Acute GVHD incidence significantly higher for MAC leading to higher early NRM compared to RIC patients Development of cGVHD is associated with significantly lower relapse rate Disease response following DLI for relapse disease together with the impact of cGVHD suggest Graft versus WM effect Conclusions
Obtain maximum response – improve outcome Improve duration of response Prevent reduce complications – reduce late effects Maintain quality of life Professionals Industry Patients / Families Voluntary sector TREATMENT GOALS FOR WM PATIENTS