Download
1 / 29
290 likes | 294 Views
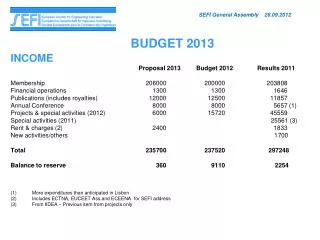
MEDICAID RESTRUCTURING BUDGET BACKGROUND February 2013. Office of Administration Division of Budget and Planning. MEDICAID RESTRUCTURING BUDGET BACKGROUND. Background Information Cost for new Medicaid eligibles Savings in state share for existing populations Additional revenue

E N D
MEDICAID RESTRUCTURINGBUDGET BACKGROUNDFebruary 2013 Office of Administration Division of Budget and Planning
MEDICAID RESTRUCTURINGBUDGET BACKGROUND • Background Information • Cost for new Medicaid eligibles • Savings in state share for existing populations • Additional revenue • Summary of budget impact • Provider payments
BACKGROUND INFORMATION • Missouri currently provides Medicaid for parents up to 19% of the Federal Poverty Level (FPL). - For a family of four, $4,475 per year. • Missouri does not provide Medicaid to non-custodial adults, unless they are disabled or seniors. • In the future, would cover low-income working adults up to 138% of the FPL. - For a family of four $32,499 annual income.
BACKGROUND INFORMATION • Missouri’s typical federal match rate for the current Medicaid Program is 62%. • Missouri provides Medicaid currently to about 900,000 Missourians: - 543,000 children; - 166,000 persons with disabilities; - 80,000 low income parents; - 76,000 low income elderly; and - 28,000 pregnant women.
COST -- STATE SHARE • No state cost for first three fiscal years (FY14-FY16). • State share then phases up to 10%: - January 2017 – 5% (half year for FY 2017); - January 2018 – 6%; - January 2019 – 7%; and - January 2020 – 10% .
MEDICAID PROJECTIONS NUMBER OF PEOPLE 307,542 292,061 276,579 268,039 259,499
COST PER PERSON • Developed by actuary • Added cost for wrap around for medically frail • Pay a commercial reimbursement rate • Savings from better care coordination (multiple avenues) • Assumes maximum cost sharing (copays) allowed
COST PER PERSON • Per Member/Per Month - $436 for parents - $583 for childless adults - $1,635 for medically frail • Trended forward at average of 4%
SAVINGS – EXISTING POPULATIONS • Current Medicaid Populations under 138% FPL • Pregnant women – covered prior to pregnancy • Ticket to Work • Breast/Cervical Cancer • Spenddown • Women’s Health Services
SAVINGS – EXISTING POPULATIONS • Current State Only Populations under 138% FPL • Blind Pension • Corrections • Dept of Mental Health Clients
SAVINGS – EXISTING POPULATIONSGENERAL REVENUE (millions of $)
ADDITIONAL REVENUE • Key Assumptions – Income Tax • No multiplier assumed • Looked at increased federal revenue to providers • Discounted to portion typically used for salaries based on individual provider-type • Applied 4.5% income tax rate
ADDITIONAL REVENUE • Key Assumptions – Sales Tax • No multiplier assumed • 19.2% of income spent on GR taxable goods • 6.9% of non-salary spent on GR taxable goods • Tax rate of 3% goes to GR
ADDITIONAL REVENUE • Key Assumptions – High Risk Pool • High Risk Pool no longer necessary • Insurance companies help fund pool through assessments • Taken as credits against taxes owed • Typically do not take full credit in first year • Fully realized ($22M), with $1.5M savings from normal growth each year after that
ADDITIONAL REVENUE$s in millions $61.8 $57.3 $53.5 $15.6
MEDICAID RESTRUCTURINGBUDGET SUMMARY • State costs for new eligibles $0 until FY 2017 • Full phase in of state share at 10% in FY 2021 • Savings for existing populations begin immediately • Additional revenue estimate conservative – no multiplier
PROVIDER PAYMENTS Hospital Reductions • Regardless of a state’s decision to expand Medicaid, payments to hospitals will be reduced. • Reductions will be to Disproportionate Share Hospital (DSH) payments. • Hospitals that serve a high percentage of Medicaid and/or other low income individuals qualify for DSH payments. • These payments are designed to help cover the cost of uncompensated care.
HOSPITAL PAYMENT REDUCTIONS • Each state’s share of the DSH reduction is unknown. • HHS Secretary will determine methodology. • That methodology to consider: • Percentage of uninsured, • State’s use of DSH funds, and • State’s current DSH level (high DSH states, like Missouri, may face a larger cut).
HOSPITAL PAYMENT REDUCTIONS • Medicaid DSH cuts at the national level: • 5% for first three years • 15% for next year • 50% thereafter • Missouri’s FY 2013 DSH payments: • $511 million hospitals • $207 million DMH hospitals
HOSPITAL PAYMENT REDUCTIONS • Hospitals will also see cuts in Medicare payments. • These payments do NOT flow through the state. • Medicare DSH cuts comparable to Medicaid. • Medicare direct inpatient payments will also be reduced (reduction in trend).
PROVIDER PAYMENTSMEDICAID RESTRUCTURING Estimated payments by provider type: • 49% ($900 million) professional services • 13% ($240M) mental health • 11% ($200M) physician services • 9% ($160 M) in-home • 16% ($300M) other (DME, ambulance, ….) • 40% ($740 million) hospital services • 11% ($200 million) pharmacies
CONCLUSION • Restructuring Medicaid has a net positive impact on the budget • Cuts to hospital payments will happen • Those reductions will be mitigated through increased provider payments, if restructure • Other considerations - indirect budget implications: • Improved access to care • Better health outcomes • Improved job retention when healthy • Reduce cost shift to private premiums