Download
1 / 11
160 likes | 228 Views
Protein C deficiency 25/12/2010. BY: MOHAMMED ALSAIDAN. Protein C deficiency. AR, usually presents in the neonatal period with purpura fulminans (PF) severe disseminated intravascular coagulation (DIC) venous thromboembolism (VTE) Asymptomatic : 1 in 500 healthy individuals

E N D
Protein C deficiency 25/12/2010 BY: MOHAMMED ALSAIDAN
Protein C deficiency • AR, usually presents in the neonatal period with • purpurafulminans (PF) • severe disseminated intravascular coagulation (DIC) • venous thromboembolism (VTE) • Asymptomatic : 1 in 500 healthy individuals • clinically significant : 1 in 20 000 • Most parents of infants with severe protein C deficiency are asymptomatic
Protein C • Protein C is a vitamin K-dependent coagulation protein • Synthesized in hepatocytes • Activated after complex formation with thrombin on the endothelial cell receptor • It cleaves critical sites in the activated procoagulant factors V and VIII, thus inactivating these enzymes
Protein C level • Mild , moderate sever • The mean level in a healthy term infant is 40 IU /dL • lower limit of normal in infants of 25 IU /dL • Later: approximately 60 IU/dL
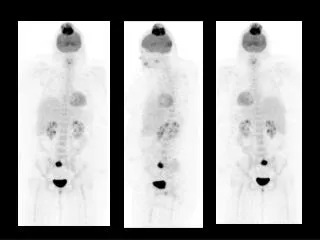
Labs • At the ontset of skin lesions: • normal Coagulation studies • elevated D-dimer • undetectable plasma protein C activity • Rapidly after onset of PF : • thrombocytopenia • hypofibrinogenaemia • prolongation of the PT
Clinical features • Foetal demise or die from DIC before diagnosis • Most affected infants are congenitally blind from thrombosis into the developing vitreal vein • Evidence of prenatal arterial ischaemic stroke on MRI • Recurrent episodes of PF triggered by infection, trauma, and minor decreases anticoagulation
Protein C deficiency • PF originates with red or purpuric lesions at pressure points • Histologically, PF lesions consist of fibrin clots in small venules of the subcutaneous fat. • Low INR short-term bridging anticoagulation with low-molecular-weight heparin or protein C replacement with concentrate, to prevent VTE, DIC and PF
Protein C deficiency • No anticoagulation required when plasma protein C concentrations above 50% around surgery and above 20% during baseline conditions • Infants managed with intensive anticoagulation and/or protein C replacement have exhibited normal growth in longterm follow-up • Some will have developmental delays and/or cognitive impairment
K H T A N Y U O