Download
1 / 20
220 likes | 417 Views
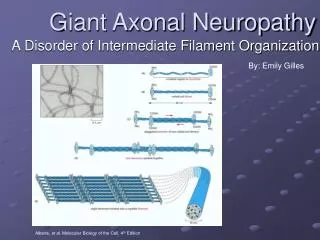
By: Emily Gilles. Giant Axonal Neuropathy. A Disorder of Intermediate Filament Organization. Alberts, et al . Molecular Biology of the Cell, 4 th Edition. Normal Intermediate Filaments. Provide mechanical strength Not all cells have IFs. Different cell types have different types of IFs.

E N D
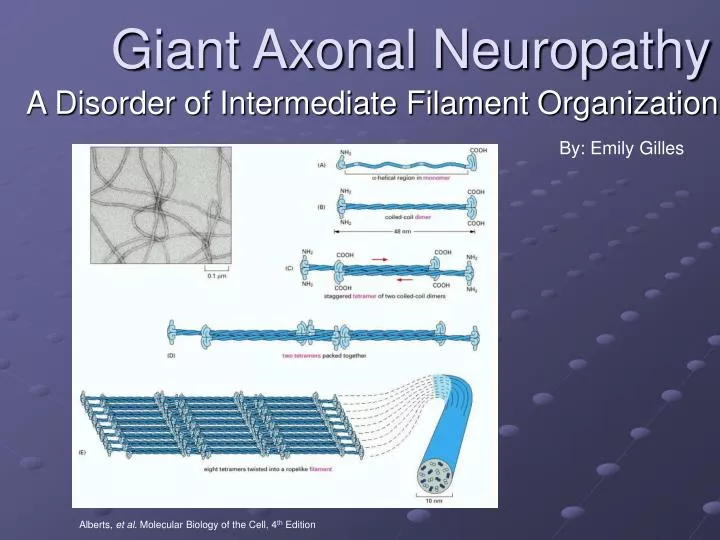
By: Emily Gilles Giant Axonal Neuropathy A Disorder of Intermediate Filament Organization Alberts, et al. Molecular Biology of the Cell, 4th Edition
Normal Intermediate Filaments • Provide mechanical strength • Not all cells have IFs. • Different cell types have different types of IFs. • Keratin is the IF in endothelial cells • Neurofilaments are found in the axons of neurons • Lamins are found lining the nuclear lamina of some cells • Vimentin is found in cells of mesenchymal origin Alberts, et al. Molecular Biology of the Cell, 4th Edition
Disease vs. Control Axon • (a) = GAN patient • Closely packed neurofilaments, peripheral cluster of microtubules Timmerman, et al. Nature Genetics26(3):254-255 (2000). • (b) = control • Homogenous distribution of neurofilaments and microtubules
Diagnosis = Sural Nerve Biopsy The pathological hallmark is the disorganization of the intermediate filament network of the cytoskeleton, with axons being predominantly affected. Control GAN
The typical clinical case: • Disease onset typically occurs between ages 4-7. • Death occurs before the age of 30. • Symptoms begin as clumsiness of gait and progressive weakness starting at the lower limbs. • Dysarthria, nystagmas, facial weakness, and mental retardation soon become apparent. • Kinky hair may or may not be present. • Rare, autosomal recessive Maia, et al. Neuropediatrics19(1):10-15 (1988). Treiber-Held, et al. Neuropediatrics25(2):89-93 (1994).
Homozygosity Mapping • What is homozygosity mapping? • Exactly like positional cloning • Fewer affected individuals can be used • Offspring must be from consanguineous parents In addition to being homozygous at the disease allele, there is a greatly increased likelihood of being homozygous by descent in adjacent regions of the genome. Ben Hamida, et al. Neurogenetics1(2):129-133 (1997). Flanigan, et al. Annals of Neurology43(1):143-148 (1998).
Refinement of the GAN locus Cavalier, et al. European Journal of Human Genetics8(7):527-534 (2000).
The Gene: Gigaxonin Bomont, et al. Nature Genetics26(3):370-374 (2000).
Expression is Ubiquitous Bomont, et al. Nature Genetics26(3):370-374 (2000). RT-PCR was used to amplify RNAs from mouse tissues. The probe used to detect was the EST aa726805.
Disease-Causing Mutations Bomont, et al. Nature Genetics26(3):370-374 (2000).
Additional Mutations Discovered Bomont, et al. Human Mutations21(4):446-451 (2003). Kuhlenbaumer, et al Neurology58(8):1273-1276 (2002).
Cytoskeletal Elements are Cross-Linked • Actin filaments, microtubules, and intermediate filaments interact via cross-linking proteins • Picture below shows intermediate filaments (blue) linked to microtubules (red) via plectin (green) Alberts, et al. Molecular Biology of the Cell, 4th Edition
Yeast Two-Hybrid Setup • Blue circle = DNA binding domain • Yellow square = gigaxonin • Red square = protein from human brain cDNA • Blue semi-circle = activator domain Criekinge WV and Beyaert R. Biological Proceedures Online2:1-38 (1999)
Gigaxonin colocalizes with MAP1B-LC • HA-Gig and flag-MAP1B-LC were cotransfected into cos7 cells • Gigaxonin and MAP1B-LC colocalize together • D shows diffuse accumulation of gigaxonin in cytoplasm when transfected alone Ding, et al. Journal of Cell Biology158(3):427-433 (2002).
In vivo Results Similar to in vitro • Gigaxonin colocalizes with MAP1B-LC in vivo. Ding, et al. Journal of Cell Biology158(3):427-433 (2002).
Functional Significance A = depolymerized microtubules within 15 min of colchicine treatment (untransfected cells) B = depolymerized microtubules within 60 min of colchicine treatment (single transfected cells) C and D = Intact network after 2 hr colchicine treatment (double transfected cells) Ding, et al. Journal of Cell Biology158(3):427-433 (2002).
Molecular Diagnosis/Treatment • Molecular Diagnosis is only available on a research basis. • There is no cure and treatment is based on alleviating treatable symptoms. Current diagnosis based on: • nerve biopsy showing thinly myelnated, enlarged axons • nerve conduction studies showing reduced nerve conduction velocity (NCV), severely reduced compound motor action potentials (CMAP) and absent sensory nerve action potentials (SNAP) • abnormal visual evoked responses • EEG showing increased slow wave activity • MRI showing cerebellar and white matter abnormalities
Summary • Giant Axonal Neuropathy is a rare, autosomal recessive disease. Diagnosis is mainly based on the appearance of giant axons containing aggregated neurofilaments in a sural nerve biopsy. • The disease locus was mapped to chromosome 16q21 by homozygosity mapping. • Using additional markers the disease locus was refined to a smaller, 590kb region. • Gigaxonin was identified by searching an EST database. cDNA of the gene was cloned from a cDNA human brain library. • Several different point mutations throughout the gene can result in the disease phenotype. • Gigaxonin binds to MAP1B-LC, as determined fluorescently tagged antibodies and immunoprecipitations. This interaction improves the stability of the microtubule network. • Molecular treatment cannot be addressed until more is known about the gigaxonin gene product.
References Alberts, et al. Molecular Biology of the Cell, 4th Edition Ben Hamida, et al. Neurogenetics1(2):129-133 (1997). Bomont, et al. Human Mutations21(4):446-451 (2003). Bomont, et al. Nature Genetics26(3):370-374 (2000). Cavalier, et al. European Journal of Human Genetics8(7):527-534 (2000). Criekinge WV and Beyaert R. Biological Procedures Online2:1-38 (1999) Ding, et al. Journal of Cell Biology158(3):427-433 (2002). Flanigan, et al. Annals of Neurology43(1):143-148 (1998). Kuhlenbaumer, et al Neurology58(8):1273-1276 (2002). Maia, et al. Neuropediatrics19(1):10-15 1988. Timmerman, et al. Nature Genetics26(3):254-255 (2000). Treiber-Held, et al. Neuropediatrics25(2):89-93 (1994).
Identifying Gigaxonin Binding Partners • Ubiquitous expression was confirmed with immunoblot • Transfected cos7 cells expressed gigaxonin • HA epitope tag at C- and N- terminal was recognized by α-HA antibody Ding, et al. Journal of Cell Biology158(3):427-433 (2002).