Download
1 / 34
340 likes | 545 Views
Amphotericin- or Echinocandin-Based Antifungal Prophylaxis Approaches. Jo-Anne Young, MD, FACP, FIDSA. Disclosures. Clinical Trials funding support (antifungal agents): Pfizer, Astellas, Merck, Schering-Plough

E N D
Amphotericin- or Echinocandin-Based Antifungal Prophylaxis Approaches Jo-Anne Young, MD, FACP, FIDSA
Disclosures • Clinical Trials funding support (antifungal agents): Pfizer, Astellas, Merck, Schering-Plough • Clinical Trials funding support (outside of mycology): Glaxo, ViroPharma, Advanced Biologics, Adamas • Not a Consultant • Not on a Speaker’s Bureau
Objectives • Amphotericin as antifungal prophylaxis • Merits, Problems • Echinocandins as antifungal prophylaxis • Merits, Problems • Undefined areas in practice
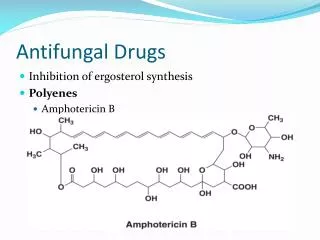
Amphotericin routes • Oral • ICU Selective digestive tract decontamination • Radiotherapy lung cancer patients • Nebulization or nasal spray • Lung transplant • HSCT • IV
Standard care • SDD consisted of 4 days of intravenous cefotaxime and topical application of tobramycin, colistin, and amphotericin B in the oropharynx and stomach. • SOD consisted of oropharyngeal application only of the same antibiotics.
Nonrandomized study of lung cancer consecutive patients • 20 patients 67 Gy (range 61-80 Gy) AmB QID from day 8 to the end of radiotherapy • Trend toward higher esophageal volumes • Older • Worse median Karnofsky Index • More often received induction chemotherapy • Start of symptoms day 21 (median, range 14-44) • 5 patients developed esophagitis grade 1 • 20 patients 60 Gy (range 51-67.5 Gy) control group • Start of symptoms day 18 (median, range 10-32) • 14 patients showed esophagitis grade 1 and 2 patients grade 2 (p < 0.05).
Nasal • Bottle design to prevent aspiration of nasal secretions back into the bottle • Each nostril 5x/day • Compliance a problem • Irritating to nasal mucosa: tolerance a problem • Reduction in surveillance CFUs, but not in invasive disease
Bronchial Anastamosis Courtesy of Jordan Dunitz, MD
6 single and 6 double lung recipients • One 7-ml (35 mg) nebulized dose labeled with Technetium
Selected system: AeroEclipse nebulizer & DeVilbiss compressor
3.9 + 1.6 mg allograft, 2.1 + 1.1 mg native 2.8 + 0.8 mg Left, 4.0 + 1.3 mg Right
271 patients 407 neutropenic episodes. Some adverse effects, but none serious, in the liposomal amphotericin B group were reported, most frequently coughing (16 patients vs. 1 patient; P=.002). Prophylactic inhalation of liposomal amphotericin B significantly reduced the incidence of IPA.
Intent-to-treat analysis • 18 of 132 patients in the placebo group developed IPA • 6 of 139 patients in the liposomal amphotericin B group • odds ratio, 0.26; 95% CI, 0.09-0.72; P=.005 On-treatment analysis • 13 of 97 patients receiving placebo developed IPA • 2 of 91 receiving liposomal amphotericin B • odds ratio, 0.14; 95% CI, 0.02-0.66; P=.007
Nebulization: merits • Directed delivery to the lungs, good distribution throughout lung airways • Achieves high local concentration • Half-life in lung of 4.8 days • Not associated with a decline in PFTs • Avoids undesirable systemic effects and drug interactions • Lipid formulations • Penetrate the lung better • Have a longer half-life • Administer at long intervals • No demonstrated resistance
Nebulization: problems • Some increased risk of • Transient cough • Nausea • Aftertaste • Deoxycholate detergent may have adverse effects on surfactant • Breakthrough invasive disease • Pulmonary • Cerebral
Nebulization: undefined areas • Many type of nebulizers • Only a few dosages studied • No data regarding • Long term efficacy • Repeated use efficacy • Comparison to systemic antifungals • Synergy with systemic antifungals • Lack of standardization of administration procedures and doses • These are not treatment data
IV • Potential systemic toxicity • Amphotericin accumulates in the reticulo-endothelial system • Even a single dose may proved tissue depots for prophylaxis in at-risk pts such as liver transplant • Intermittent high dosing of lipid ampho may be an option to daily azoles or candins
Enrollment was discontinued in the SCT group as recommended by the independent data review committee in accordance with the 10% limit of AEs (CTC grade 3-4) fixed by the protocol.
Randomized, double-blind Phase III study • 72 centers in the US and Canada • Patient population: • HCT candidates 6 months of age • Autologous HCT for heme malignancies only CID 2004;39:1407-16 (van Burik et al.)
Treatment success Treatment difference Micafungin 340 / 425 (80%) +6.5% P=0.03 (95% CI, 0.9% to 12%) Fluconazole 336 / 457 (73.5%) • Assess non-inferiority of micafungin to fluconazole over 10% • Treatment success • Absence of suspected, proven, or probable invasive fungal infection through the end of prophylaxis period • Absence of a proven or probable invasive fungal infection through the end of the 4-week post-treatment period
Time to Treatment Failure Proportion of Patients with Treatment Success P-Value (2 tailed) = 0.025 Days Since First Dose of Study Drug
P=0.07 Micafungin compared with Fluconazole Breakthrough fungal infection Aspergillus* Proven Probable Candida Fusarium Zygomycetes Death Death due to FI Micafungin 7/425 (1.6%) 1 0 1 4 1 1 18/425 (4.2%) 1 (Zygomycetes) Fluconazole 11/457 (2.4%) 7 4 3 2 2 0 26 / 457 (5.7%) 2 (Pulmonary aspergillosis)
HSCT candidates 6 months of age MicafunginFluconazole Pediatric <16 yrs 69% (27/39) 53% (24/45) Adult 16-64 yrs 81% (313/386) 76% (312/412) Adult > 64 yrs 97% (32/33) 70% (16/23)
High dose micafungin • Adult patients • Micafungin 150 mg (n = 52) orFluconazole 400 mg (n = 52) • Success 94 vs. 88% • Empirical antifungal therapy (P = 0.06)2/50 (4.0%) micafungin 6/50 (12.0%) fluconazole arm Int J Hematol. 2008 Dec;88(5):588-95
Liver transplant • Open-label trial of 71 adult liver transplant recipients • Caspofungin for at least 21 days • 2 IFI: Mucor and Candida albicans surgical wound infections • 6 discontinued: drug-related altered liver function • 8 patients died, 6 during caspofungin administration and 2 during follow-up period, but none were attributed to IFI or caspofungin toxicity Transplantation 2009 Feb 15;87(3):424-35
Echinocandins: undefined areas • Limited amount of published data: • Randomized trials • Observational cohorts • Specific patient populations • By disease • By age • Can trials with one drug be extrapolated to other drugs • Dosage
Summary • Amphotericin as antifungal prophylaxis • Merits, Problems • Echinocandins as antifungal prophylaxis • Merits, Problems • Undefined areas in practice