Download
1 / 38
380 likes | 558 Views
Epinephrine auto injectors. Anaphylactic Reaction Protocol Changes Aaron J. Katz, AEMT-P, CIC. Overview. Not just “Any allergic reaction”! Once you see it – you’ll never forget it! Reactions tend to worsen with each “exposure” You have a responsibility to educate patients and families.

E N D
Epinephrine auto injectors Anaphylactic Reaction Protocol Changes Aaron J. Katz, AEMT-P, CIC
Overview • Not just “Any allergic reaction”! • Once you see it – you’ll never forget it! • Reactions tend to worsen with each “exposure” • You have a responsibility to educate patients and families
Some interesting cases • Post Dental Visit • Bee Sting (2 cases) • Cookies with hidden nuts • Milk – 6 month old • Milk – 2 year old • Touched the fish • Penicillin shots • Allergy injections • The cheese danish • Neighborhood “X”
Introduction • Anaphylactic shock is a potentially life threatening emergency • This condition has a high mortality rate when not recognized and treated early • With allergies increasing, mortality has also increased • We don’t know why allergies are increasing
Introduction Cont. • Hatzoloh responds to approximately 400 calls per year for anaphylaxis of which 15% are of patients with true anaphylactic shock • Patients in anaphylactic shock are those that benefit from epinephrine injections • ALS units are not always readily available • More of a problem for FDNY/EMS?
Introduction • Many studies have shown that the use of an EPI- PEN can be safely administered by an EMT • The EMT must be appropriately trained
Goals • Early recognition of anaphylaxis • Early BLS intervention • Early ALS intervention • Administration of Epinephrine using the Epi-Pen Auto injector
Anaphylaxis • Allergic reaction – immune response to any substance. • Reaction can be localized or severe and life threatening (anaphylaxis) • Allergen – substance that causes the immune response
Common allergens • Insects – bees, wasps • Food – nuts, fish, milk, chocolate • Plants – poison ivy, oak • Medications – antibiotics • Other – outdoor allergens, fragrances • Latex
Skin • Swelling to face, neck, hands, feet, tongue and periorbitally • Urticaria – hives • Itching • Erythema – redness • Flushed skin • Warm tingling feeling to face, mouth, chest, feet and hands
Respiratory system • Tightness to throat and chest • Cough • Tachypnea • Labored breathing • Hoarseness • Noisy breathing – stridor or wheezing • bronchoconstriction
Cardiovascular system • Tachycardia • Vasodilation • Hypotension • Poor cardiac output!
Other systems • Itchy, watery eyes • Headache • Sense of impending doom • Runny nose, nasal congestion • Decreased mental status • Abdominal distress
Critical Point • Findings that reveal hypoperfusion (shock), or respiratory distress (upper airway obstruction, lower airway disease, severe bronchospasm ) may indicate the presence of a severe allergic reaction (anaphylaxis)
Past Treatment Protocol • Perform initial assessment • Perform focused history and physical exam, including: • History of allergies • What was patient exposed to • How were they exposed • Effects • Time of onset • Progression • interventions
Past Treatment Cont. • Assess baseline vital signs and SAMPLE history • Administer high concentration oxygen • Monitor breathing for adequacy • Request ALS assistance • Assist the patient with self-administration of their own prescribed Epinephrine • Loosen restrictive clothing or jewelry • Assess for shock and treat if appropriate
New Treatment Protocolpatients over age 9 or weighing over 30 kilos • Determine that patients history includes past history of anaphylaxis, severe allergic reactions, and/or recent exposure to an allergen • Administer high concentration oxygen • Request ALS assistance • Assess the cardiac and respiratory status of the patient
Continued • If both the cardiac & respiratory status of the patient are normal, initiate transport • If either the cardiac or respiratory status of the patient is abnormal, proceed as follows:
Continued • If the patient has severe respiratory distress or shock and has a prescribed Epi-Pen assist the patient in administration • If the auto injector is not available or expired and the EMS agency carries one, administer (0.3 mg.) as authorized by the agency medical directors • If the patient does not have a prescribed Epi-Pen, begin transport and contact medical control for authorization to administer 0.3 mg via auto injector
Note • If unable to make contact with on-line medical control and the patient is under 35 years old, you may administer 0.3 mg epinephrine via an auto-injector if indicated. • The incident should be reported to medical control or your medical director as soon as possible
Protocol cont. • Contact medical control for authorization to administer a second dose if needed • Refer to other protocols as needed (resp distress/failure, obstructed airway, shock) • If patient arrests treat as per the non-traumatic cardiac arrest protocol
Pediatric differences • The age for pediatrics in this protocol is patients under 9 years old or weighing less than 30 kg (66 lbs) • The dose of epinephrine is 0.15 mg • It can not be given without medical control authorization
Pharmacology - Epinephrine • Medication name: • Generic – Epinephrine • Trade – Adrenalin
Pharmacology – Epinephrine cont • Properties • Bronchodilation • Vasoconstriction
Indications • Must meet the following three criteria • Patient must exhibit findings of severe allergic reaction (anaphylaxis) • Medication is prescribed for this patient by their physician, direction by medical control, or inability to contact medical control and epinephrine is indicated • Administration of medication is authorized by REMAC or a physician
Contraindications • None when used to treat anaphylaxis
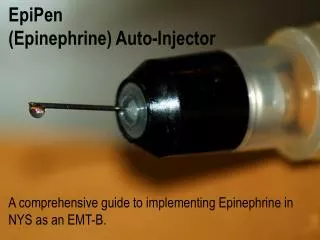
Medication form • Liquid contained in an auto injector needle and syringe system
Dosage • Adult- one adult auto injector (0.3 mg) • Infant and Child- one auto injector (infant/child) 0.15 mg
Administration • Obtain order from medical control either on line or as per protocol • Obtain patients prescribed unit if available • Ensure prescription is written for patient • Ensure medication is not discolored • Remove safety cap from device
Administration cont. • Place tip of device against the patients thigh: • Use lateral portion of thigh midway between the waist and knee • Push firmly until the injector activates • Keep in contact for 10-15 seconds • Record activity and time • Dispose of injector in appropriate container • Can be administered through patients clothes
Actions • Dilates the bronchioles • Constricts blood vessels
Side effects • Increased heart rate • Pallor • Dizziness • Chest pain/ sudden death • Headache • Nausea/ vomiting • Excitability, anxiousness
Reassessment • Continually assess ABC’S for signs of worsening patient condition such as: • Mental status change • Increased respiratory rate • Decreasing B/P
Reassessment • Be prepared to initiate BCLS measures if indicated including: CPR, AED, ALS intercept • Treat for shock • As the drug lasts in the system 10-20 minutes, be prepared for a potential return of the anaphylactic reaction
Reassessment • As many as 25% of those having an anaphylactic reaction will have a recurrence of life threatening symptoms within hours of the first attack
Transportation Decision • Any patient who received Epinephrine should be transported to an Emergency Room for evaluation • On-Line Medical Control must be contacted for any patient refusing treatment or transportation after treatment with Epi.
Special Consideration • A BLS crew may encourage an authorized layperson to administer an Epi-Pen to a patient if all of the following conditions are met: • The BLS unit is not equipped with an Epi-Pen • The Patient is having an anaphylactic reaction where Epi-Pen is indicated • ALS assistance is not readily available • An authorized layperson is present with an Epi-Pen and in the clinical judgment of the EMTs it is in the best interests of the patient to allow the authorized layperson to administer the Epi-Pen