Download
1 / 1
10 likes | 195 Views
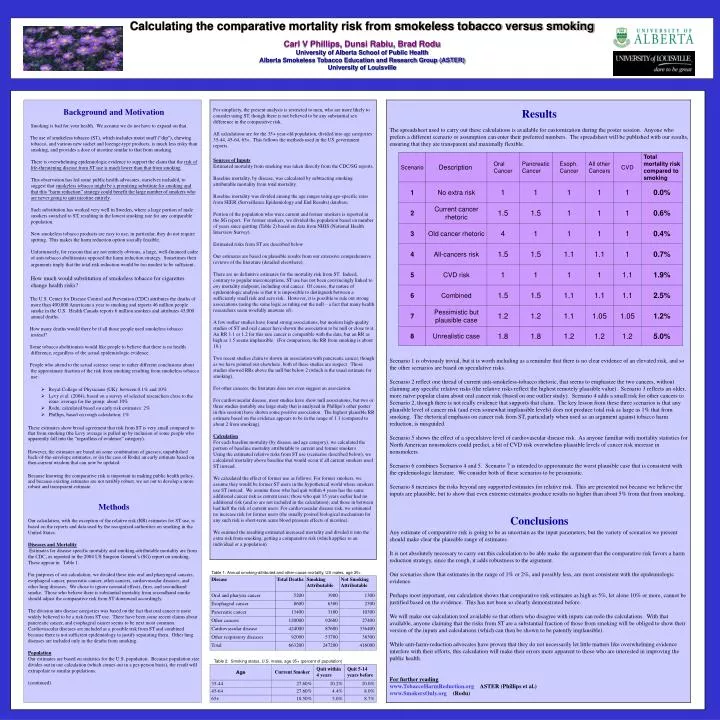
Calculating the comparative mortality risk from smokeless tobacco versus smoking Carl V Phillips, Dunsi Rabiu, Brad Rodu University of Alberta School of Public Health Alberta Smokeless Tobacco Education and Research Group (ASTER) University of Louisville. Background and Motivation

E N D
Calculating the comparative mortality risk from smokeless tobacco versus smoking Carl V Phillips, Dunsi Rabiu, Brad Rodu University of Alberta School of Public Health Alberta Smokeless Tobacco Education and Research Group (ASTER) University of Louisville • Background and Motivation Smoking is bad for your health. We assume we do not have to expand on that. The use of smokeless tobacco (ST), which includes moist snuff (“dip”), chewing tobacco, and various new sachet and lozenge-type products, is much less risky than smoking, and provides a dose of nicotine similar to that from smoking. There is overwhelming epidemiologic evidence to support the claim that the risk of life-threatening disease from ST use is much lower than that from smoking. This observation has led some public health advocates, ourselves included, to suggest that smokeless tobacco might be a promising substitute for smoking and that this “harm reduction” strategy could benefit the large number of smokers who are never going to quit nicotine entirely. Such substitution has worked very well in Sweden, where a large portion of male smokers switched to ST, resulting in the lowest smoking rate for any comparable population. New smokeless tobacco products are easy to use; in particular, they do not require spitting. This makes the harm reduction option socially feasible. Unfortunately, for reasons that are not entirely obvious, a large, well-financed cadre of anti-tobacco abolitionists opposed the harm reduction strategy. Sometimes their arguments imply that the total risk reduction would be too modest to be sufficient. How much would substitution of smokeless tobacco for cigarettes change health risks? The U.S. Center for Disease Control and Prevention (CDC) attributes the deaths of more than 400,000 Americans a year to smoking and reports 46 million people smoke in the U.S. Health Canada reports 6 million smokers and attributes 45,000 annual deaths. How many deaths would there be if all those people used smokeless tobacco instead? Some tobacco abolitionists would like people to believe that there is no health difference, regardless of the actual epidemiologic evidence. People who attend to the actual science come to rather different conclusions about the approximate fraction of the risk from smoking resulting from smokeless tobacco use: • Royal College of Physicians (UK): between 0.1% and 10% • Levy et al. (2004), based on a survey of selected researchers close to the issue: average for the group: about 10% • Rodu, calculated based on early risk estimates: 2% • Phillips, based on rough calculation: 1% These estimates show broad agreement that risk from ST is very small compared to that from smoking (the Levy average is pulled up by inclusion of some people who apparently fall into the “regardless of evidence” category). However, the estimates are based on some combination of guesses, unpublished back-of-the-envelope estimates, or (in the case of Rodu) an early estimate based on then-current wisdom that can now be updated. Because knowing the comparative risk is important in making public health policy, and because existing estimates are not terribly robust, we set out to develop a more robust and transparent estimate. Methods • Our calculation, with the exception of the relative risk (RR) estimates for ST use, is based on the reports and data used by the recognized authorities on smoking in the United States. • Diseases and Mortality Estimates for disease specific mortality and smoking-attributable mortality are from the CDC, as reported in the 2004 US Surgeon General’s (SG) report on smoking. These appear in Table 1. For purposes of our calculation, we divided these into oral and pharyngeal cancers, esophageal cancer, pancreatic cancer, other cancers, cardiovascular diseases, and other lung diseases. We chose to ignore neonatal effects, fires, and secondhand smoke. Those who believe there is substantial mortality from secondhand smoke should adjust the comparative risk from ST downward accordingly. The division into disease categories was based on the fact that oral cancer is most widely believed to be a risk from ST use. There have been some recent claims about pancreatic cancer, and esophageal cancer seems to be next most common. Cardiovascular diseases are included as a possible risk from ST and combined because there is not sufficient epidemiology to justify separating them. Other lung diseases are included only in the deaths from smoking. Population • Our estimates are based on statistics for the U.S. population. Because population size divides out in our calculation (which comes out in a per-person basis), the result will extrapolate to similar populations. • (continued) . Table 1: Annual smoking-attributed and other-cause mortality, US males, age 35+ Table 2: Smoking status, U.S. males, age 35+ (percent of population)