Download
1 / 54
660 likes | 1.98k Views
Acquired Macular Disorders. April 01, 2008. Idiopathic Central Serous Chorioretinopathy (ICSC). Transient episodes of serous retinal or RPE detachments in the macula. No predisposing retinal signs Drusen. ICSC: Characteristics. Male, caucasian, 25 to 45 years old Unilateral

E N D
Acquired Macular Disorders April 01, 2008
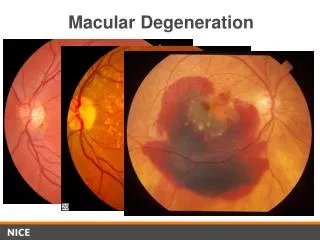
Idiopathic Central Serous Chorioretinopathy (ICSC) • Transient episodes of serous retinal or RPE detachments in the macula. • No predisposing retinal signs • Drusen
ICSC:Characteristics • Male, caucasian, 25 to 45 years old • Unilateral • Type A personality • Vascular excitability creating a localized breakdown in choriocapillaris blood supply to the RPE.
ICSC:Clinical Appearance • BIO: • Dome of elevated retina • Look for color variations, reflections off the ILM, loss of FLR • Fundus lens: • Retinal vessels within the CSR area will cast shadows onto the attached RPE. • Yellow precipitates – poorer prognosis.
Chronic ICSC:Precipitates “Lemon-drop nodules”
ICSC:Clinical Findings • Fairly sudden visual acuity reduction. • 20/40 • A hyperopic refractive shift. • Relative scotoma, metamorphopsia, micropsia, and impaired dark adaptation.
ICSC: • About 80% of ICSC cases spontaneously resolve in 6 months. • Mild metamorphopsia can remain. • Permanent visual acuity reduction or disturbance. • prolonged detachment or recurrent attacks • 20% recurrent rate • Focal laser if VA decrease is significant.
ICSC:Other Diagnostic Testing • Fluorescein angiography • typically shows a 'smokestack' and 'umbrella' or 'mushroom' hyperfluorescence (late venous phase) • OCT
ICSC: OCT
CME • Accumulation of fluid within the macula. • Layers affected typically are the outer plexiform (Henle's fiber) layer and the inner nuclear layer. • Macular thickening occurs with multiple cystic areas.
CME:Causes • Post-op cataract (Irvine –Gass syndrome) • Post YAG capsulotomy • Retinal surgery • Intraocular inflammation • Retinal vascular conditions
CME: Clinical Appearance • Often seen as just a loss of the FLR • Prolonged photostress recovery test • Any other clinical tests?
CME:Fluoroscein angiography • Petalliform appearance
CME: OCT
CME:Management • Depends on underlying cause: • Laser photocoagulation vascular cases (i.e. retinal vein or arterial occlusions • Steroids and non-steroidal anti-inflammatory drugs (Triamcinolone)
ERM: • AKA - premacular gliosis, cellophane maculopathy, surface-wrinkling retinopathy, preretinal fibrosis, and macular pucker • Occur as the result of proliferation of retinal glial cells on the ILM that have escaped through breaks in the ILM.
ERM:Treatment • Vitrectomy and membrane peeling • indicated only if significantly reduced visual acuities.
ERM: Vitrectomy and membrane peeling
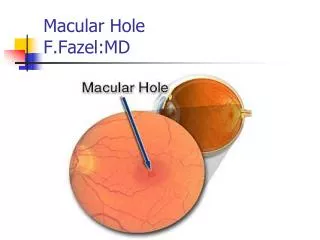
Macular holes: • Results from a perifoveal focal vitreous cortex contraction. • pulls the macular tissue free from the choroid. • typically spontaneous and abrupt • bilateral in only 10 percent of cases.
Etiologies of macular hole: • Idiopathic (affects mainly postmenopausal women) • Severe Myopia (associated with posterior staphylomas) • Trauma (vitreous traction or commotio retinae) • Solar Retinopathy (very small lamellar hole or cyst, 2 weeks post-UV exposure
Stages of macular holes: Stage 1: Decreased or absent foveal depression. Small round yellow spot/ring in fovea. Macular cyst Stage 2: Tangental tear at one edge of fovea.
Stages of macular holes: Stage 3: Round punched-out area about 1/3 disc diameter. Halo of retinal detachment surround. Visual acuity usually 20/200 or worse. Stage 4: Complete hole Edematous ‘cuff’ at margins
Macular hole stages: 1 2 3 4
Treatment of Macular holes Treatment of macular holes involve ILM peeling and vitrectomy. • relieves vitreo-retinal traction • stimulates glial cell proliferation and migration into the macular area
Toxic maculopathies • Exogenous substances causing potential toxicity to the macula. • Antimalarials • Phenothiazines • Tamoxifen • Talc
Plaquenil (Hydroxychloroquine): • Used to treat malaria and rheumatological disorders (i.e. rheumatoid arthritis, lupus). • Tends to concentrate in melanin-containing structures such as the RPE and choroid • Excess of 300g cumulative oral dose (250mg/day for 3 years) significantly increases risk of maculopathy.
Plaquenil Maculopathy: • Classically presents as "bullseye" maculopathy. • A pre-treatment baseline retinal evaluation: • Visual acuities • Amsler grid • Color vision • Visual fields (10-2, Macular Threshold) • Dilated retinal examination • Fundus photos • Post-treatment evaluations repeated every 6 to 12 months.
Plaquenil Maculopathy: • VA ranges: • 20/30 to 20/40 BCVA • faint halo of RPE pallor • 20/60 to 20/80 BCVA • dark ring surrounds halo (Bull’s eye macula) • VF changes: • Scotoma to red target between 4-9 degrees.
Plaquenil maculopathy: • 10-2 HVF • Red Target
Phenothiazine: • Thioridazine (Melleril) • normal dose is 150 to 600mg/day • greater than 800mg/day for a few weeks can cause retinotoxicity • Chlorpromazine (Largactil) • normal is 75 to 300mg/day • greater than 2400mg/day over many weeks can cause retinotoxicity
Phenothiazine Maculopathy: • Retinopathy presents as a “salt and pepper” appearance to the macula. • A coarse granular macular pigmentation • usually appears first • Decreased visual acuities and poor dark adaptation. • May not progress if drug is discontinued. • Geographic RPE/choriocapillaris atrophy with hyperpigmented clumps with continued drug use.
Tamoxifen: • (Nolvadex, Emblon, Noltam, Tamofen) • is an anti-estrogen used to treat breast carcinoma. • normal dose of 20 to 40mg/day • current dosages prescribed today are usually less.
Tamoxifen Maculopathy: • Presents as multiple superficial yellow crystalline ring-like deposits at the macula. • can cause visual acuity loss • Also – A vortex keratopathy and optic neuritis can rarely occur.