Download
1 / 14
310 likes | 3.95k Views
Atelectasis. Causes : airway obstruction with mucus and solid object Lack of surfactant in fluids lining the alveoli Effects : Lung collapse lead to compression of veins increase blood flow resistance Additional vasoconstriction due to hypoxia in collapsed alveoli. Atelectasis.

E N D
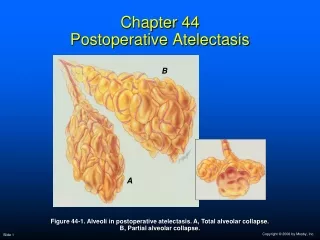
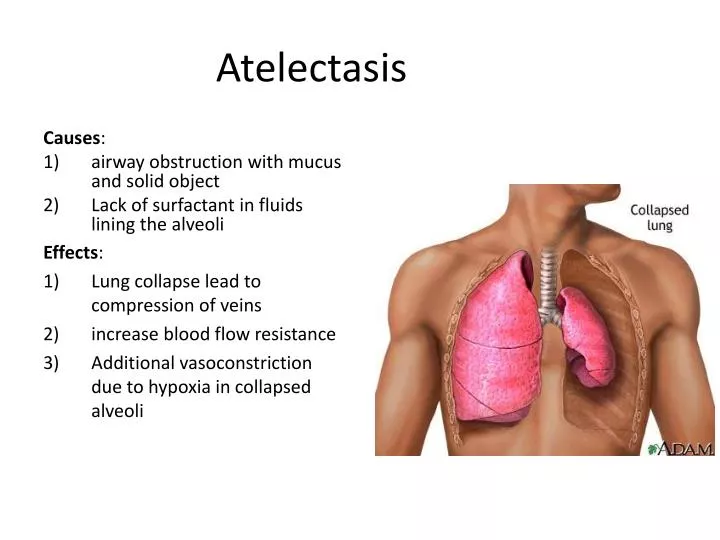
Atelectasis Causes: • airway obstruction with mucus and solid object • Lack of surfactant in fluids lining the alveoli Effects: • Lung collapse lead to compression of veins • increase blood flow resistance • Additional vasoconstriction due to hypoxia in collapsed alveoli
Atelectasis • Vasoconstriction lead to decrease blood flow through Atelectasislung: • 1)blood5/6 passes to aerated lung • 2)Blood 1/6 passes to unaeratedlung • V/Q ratio is moderately compromised • only mild oxygen desaturation in aortic blood despite total loss of ventilation in an entire lung
Lack of surfactant as a cause of lung collapse • Special alveolar epithelial cells secrete surfactant leads to fluid that coat inside surface of alveoli lead to 2-10 times decrease surface tension in alveoli which prevents alveolar collapse • In case of RDS in newborn premature babies, alveoli lead to decrease surfactant result in increase surface tension lead to lung collapse patient may die due to suffocation with Atelectasis.
Tuberclosis • A constrictive lung disease Etiology: tubercle bacilli lead to tissue reaction in lungs lead to Pathology: • Macrophage invasion • Walling off of lesion by fibrous tissue leading to tubercle formation • If untreated in 3% walling off fails • Massive destruction of lung tissue • Large abcess cavities • Late stages= increase fibrous tissue and decrease function of lung tissue.
Physiologic abnormalities of tuberculosis: • Increase work of breathing by respiratory membrane • Decrease respiratory membrane surface area • Increase thickness of respiratory membrane • Decrease vital capacity • Decrease breathing capacity • Decrease pulmonary diffusion capacity • Abnormal ventilation perfusion ratio
pneumonia • It is an infection of pulmonary parenchyma. • It may involve primarily the interstium or alveoli • Caused by viruses,fungi,and parasites.
Pneumonia • Involvement of entire lobe is called LOBAR PNEUMONIA • Involvement of alveoli contiguous to bronchi is called BRONCHOPNEUMONIA
pneumonia • Abnormalities of function (Pathology): • Consolidation of lung occurs i.e, alveoli are filled with blood cells and fluids • Pulmonary membrane becomes inflamed and porous so leaking occurs. • Decrease total surface area of respiratory membrane • Decrease V/Q ratio which results in hypoxemia and hypercapnia
DYSPNEA = Air Hunger Dyspnea: shortness of breath (SOB), or air hunger, is the subjective symptom of breathlessness. 3 factors that cause the sensation of dyspnea: 1) Abnormality of respiratory gases in body fluids (mainly hypercapnia & partly hypoxia) 2) Increase work of breathingby respiratory muscles to breath forcefuly e.g. in asthma 3) State of Mind (neurogenic/emotional dyspnea) • More enhanced in people who are claustrophobic (fear of not being able to receive a sufficient quantity of air e.g., small or crowded places).
HYPERCAPNIA: DEFINITION: • Excess CO2 in body fluids. • (Hypercapnia + Hypoxia): Only when hypoxia is caused by hypoventilation or circulatory deficiency.
Causes of hypoxia + hypercapnia (simultaneously): • In hypoxia due to hypoventilation, CO2 transfer between alveoli & atmosphere is affected as much as is oxygen transfer. • In circulatory deficiency decreased blood flow decreased removal of CO2 from the tissues tissue hypercapnia + hypoxia. • But transport capacity of blood for CO2 is more than 3 times that for O2, so resulting tissue hypercapnia in much less than tissue hypoxia.
Severe hypercapnea • When alveolar PCO2 rises above about 60-75 mm Hg air hunger / dyspnea becomes severe. • If PCO2 rises to 80-100 mm Hg lethargy, +/- semicomatose • If PCO2 rises to 120 to 150 mm Hg + / - anesthesia & death • At such high PCO2 Resp. Centre is depressed rather than stimulated vicious circle
ASPHYXIA: DEFINITION: Simultanoeus acute hypoxia & hypercapnia. CAUSES: • Acute airway obstruction • When a person is forced to re-breathe his own air in a confined space.
Mechanism: • During asphyxia hypoxia + hypercapnia strong stimulation of respiratory centre & violent inspiratory efforts heart rate increases, BP increases, CATS increase from adrenal medulla (increase in nor-epinephrine > epinephrine) unconsciousness, convulsions & decrease in respiratory rate death.