Download
1 / 35
400 likes | 619 Views
Rituximab vs. Cyclophosphamide for Induction of Granulomatosis with Polyangiitis. Sukhjinder Sidhu Interior Health Pharmacy Resident Nephrology Rotation March 6, 2014. Learning Objectives. By the end of this 45-min session the audience should be able to:

E N D
Rituximab vs. Cyclophosphamide for Induction of Granulomatosis with Polyangiitis Sukhjinder Sidhu Interior Health Pharmacy Resident Nephrology Rotation March 6, 2014
Learning Objectives • By the end of this 45-min session the audience should be able to: • Describe the pathophysiology of granulomatosis with polyangiitis (GPA) • Describe the clinical presentation of GPA • Be able to explain the evidence for the treatment of GPA • Become aware of the special authority criteria for rituximab
DRPs • WB is at risk of experiencing worsening GPA symptoms and death secondary to not receiving optimal induction therapy and would benefit from initiation of induction therapy • WB has an elevated blood pressure secondary to the use of glucocorticoids and would benefit from optimization of hypertensive therapy • WB is at risk of experiencing hypoglycemia in the morning secondary to a high dose of insulin at night and would benefit from optimization of insulin management • WB is at risk of steroid-induced osteoporosis secondary to receiving too low a dose of calcium carbonate and would benefit from dose adjustment • WB is at risk of prolonged anemia secondary to a drug-drug interaction between iron sulfate and calcium carbonate and would benefit from changing administration time
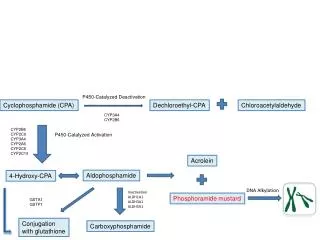
Granulomatosis with Polyangiitis • GPA aka Wegener’s • Necrotizing inflammation of small blood vessels • Classic triad of upper and lower respiratory tracts and kidneys • More commonly affecting caucasians with a male: female ratio of 1:1 • Mean age of onset ~40 years Langford CA, Fauci AS (2012). Harrison’s Principles of Internal Medicine, 18e.
Granulomatosis with Polyangiitis Autoimmun Rev. 2010 May;9(7):483-7
Granulomatosis with Polyangiitis * if new/worse – denotes a major item for assessment of flares
Granulomatosis with Polyangiitis • Diagnosis • > 2 of the following: • Abnormal urinary sediment (red cast cells or > 5 rbc/hpf) • Abnormal findings on CXR • Oral ulcers/nasal discharge • Granulomatous inflammation on biopsy • Pauci-immune, segmental necrotizing & crescentic • Consider testing for ANCA • 90-95% positive for PR3-ANCA • 5-10% positive for MPO-ANCA Langford CA, Fauci AS (2012). Harrison’s Principles of Internal Medicine, 18e. Arthritis Rheum 1990 Aug;22(8):1101
Goals of Therapy • Achieve remission • Prevent further kidney damage • Prevent further extra-renal damage/complications • Prevent relapse • Prevent mortality • Prevent adverse events
Therapeutic Approach • Corticosteroids • Methylprednisone 500 mg IV x 3 pulses, then prednisone 1 mg/kg/day PO x 4 weeks & taper over 3-4 months • Immunosuppressants • Cyclophosphamide 0.75 g/m2IV Q 3-4 weeks x 3-6 months • Cyclophosphamide 1.5-2 mg/kg/day PO x 3-6 months • Rituximab 375 mg/m2 IV weekly x 4 doses
RITUXVAS NEJM 2010;363:211-20
RITUXVAS – Baseline Characteristics NEJM 2010;363:211-20
RITUXVAS - Results Rituximab – 76% Cyclophosphamide – 82% ARR -6% (95% CI, -33 to 21; p=0.68) Rituximab – 42% (1.00/pt-year) Cyclophosphamide – 36% (1.10/pt-year) (95% CI, 0.61 to 1.99; p=0.77) NEJM 2010;363:211-20
RITUXVAS • Author’s conclusions: • The rituximab-based regimen was not superior to the conventional cyclophosphamide regimen when used as induction treatment in patients with ANCA-associated renal vasculitis
RITUXVAS • Strengths • ITT • No patient lost to follow up • All patients were newly diagnosed • Limitations • Unblinded trial • Before enrollment, patients were allowed to receive plasmapheresis or methylprednisolone 2 g IV (max) • Small patient population studied • Long term effects of induction with rituximab not known • Clinical manifestations besides renal involvement unknown • Baseline characteristics appear to be unbalanced • Relapse rates unknown • Generalizability • Included patients with rapidly progressive glomerulonephritis • Large proportion of patients had compromised GFR NEJM 2010;363:211-20
RAVE * > 1 BVAS/WG major item or severe enough to require treatment with cyclophosphamide NEJM 2010;363:221-32
RAVE – Baseline Characteristics NEJM 2010;363:221-32
RAVE - Results NEJM 2010;363:221-32
RAVE - Results * death from any cause, cancer, leukopenia , thrombocytopenia , infections , drug-induced cystitis, VTE, stroke, hospitalization, infusion reactions leading to D/C NEJM 2010;363:221-32
RAVE • Author’s conclusions: • … treatment with rituximab and glucocorticoids is not inferior to standard regimen in patients with severe ANCA-associated vasculitis of recent onset • … the regimen may be superior to the standard regimen of cyclophosphamide and glucocorticoids for remission induction in severe relapsing ANCA-associated vasculitis NEJM 2010;363:221-32
RAVE • Strengths • ITT • Maintained blinding throughout study & no patients lost to follow-up • Crossover patients/withdrawals were accounted for as treatment failures • Patients received standard of care with glucocorticoids • Limitations • Patients included had less severe disease • Powered? • ~50% of patients had relapsing ANCA-associated vasculitis with many having failed cyclophosphamide therapy • Small population studied • Short duration of therapy • Generalizability • Not all patients newly diagnosed • Majority of patients with GPA and extra-renal manifestations • Reserved renal function
KDIGO Guidelines • Cyclophosphamide and corticosteroids as initial treatment (1A) • Rituximab and corticosteroids as an alternative initial treatment in patients without severe disease or in whom cyclophosphamide is contraindicated (1B) KDIGO 2012 Clinical Practice Guideline for Glomerulonephritis
BC PharmaCare • Rituximab requires special authority • Criteria • Induction of remission in severely active GPA or MPA in patients who: • have a severe intolerance/CI to cyclophosphamide • failed an adequate trial of cyclophosphamide • Prescribed by rheumatologist, nephrologist or respirologist • Completion of BVAS
Application • Necessary • +ve ANCA, +ve renal biopsy, clinical manifestations present • Effective • Rituximab is non-inferior to cyclophosphamide in newly diagnosed GPA • Safety • Long-term safety of rituximab unknown • Patient Factors • Cost concerns and doesn’t meet SA criteria
Therapeutic Plan • Received cyclophosphamide 1 g IV • To be followed up in 4 weeks for subsequent dose • Received co-trimoxazole for PCP prophylaxis • Amlodipine 2.5 mg PO daily • Insulin glargine regimen changed to 16 units SC QAM, 9 units SC QHS • Calcium carbonate 1250 mg PO BID • Discontinued ferrous sulfate