Download
1 / 11
110 likes | 239 Views
Vastus Slide and Controlled Perforations. Instructional Course Lectures Chapter 3, Volume 48, 1999 Head, MD; Montgomery, MD; Emerson, MD Sepein Chiang, D.O. Introduction. Increasing number of revision THA More challenging and higher potential for complications than primary THA

E N D
Vastus Slide and Controlled Perforations Instructional Course Lectures Chapter 3, Volume 48, 1999 Head, MD; Montgomery, MD; Emerson, MD Sepein Chiang, D.O.
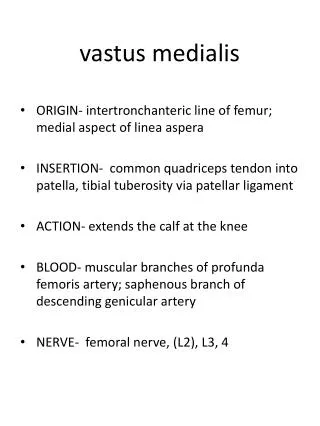
Introduction • Increasing number of revision THA • More challenging and higher potential for complications than primary THA • Cement removal is one of the more difficult aspects • Vastus slide technique provides wide exposure and access to the femur • Controlled perforations offer a safe, expedient method for cement removal
Technique • Pt is placed in the lateral decubitus position • Patellae are used as guides for leg length • Access to both the femur and acetabulum • Can be extended both proximally & distally • Anterior to posterior access to the hip joint • Allows for sciatic nerve exploration • Follow anatomic planes to avoid potential for neurovascular injury
Technique (cont) • Incision begins 10-15 cm superior & slightly posterior to the greater trochanter • Incision carried distally along the femur below the level requiring cement removal • Skin, subcutaneous tissue, iliotibial band, gluteus maximus fascia • Lateral intermuscular septum remains intact and protects the sciatic nerve
Technique (cont) • Slide technique to the gluteus medius and vastus lateralis is done thru a lazy “Z” incision • A to B, A to D are carried out in a subperiosteal fashion • Periosteal dissection carried distally, reflecting the vastus lateralis and intermedius • B to C reflects the anterior portion of the gluteus medius & minimus
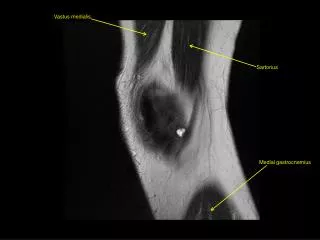
Technique (cont) • Avoid violating the abductor musculature • Superior gluteal nerve lies 4-5 cm above the greater trochanter between the gluteus medius and minimus • Externally rotate the hip and expose the hip capsule • Capsulectomy and dislocation
Technique (cont) • For cement removal the femur is externally rotated, knee flexed and the leg is dropped off the table • First removal the proximal lateral cement or run the risk of trochanteric fractures • Remove the femoral component
Technique (cont) • Midas-Rex pneumatic cutting tool to remove the cement • 5-7 cm distally, make a 7 mm perforation into the medullary canal with a Midas-Rex burr • For primary implants, 2 portals are usually sufficient
Technique (cont) • Portals are placed at least 5 cm apart • The distal portal is placed at least 2.5 cm proximal to the tip of the revision prosthesis • Portals allow the use of irrigation to remove cement debris
Conclusion • Differs from the Hardinge approach in that the substance of the abductor musculature is not invaded • Medial and posterior muscle attachments are maintained thereby preserving the blood supply to the femur • All reconstructive hip procedures can be accomplished through this surgical approach