Download
1 / 40
400 likes | 503 Views
Example of HSR project: Cardiac Counselling and Rehabilitation: RCT of Complex Interventions. Marie Johnston. ‘History’. Initiation – 1991! Expertise + experience Grant application – funded by Chief Scientist Office Differences ‘now’ Co-applicants MRC Framework for Complex Interventions

E N D
Example of HSR project:Cardiac Counselling and Rehabilitation: RCT of Complex Interventions Marie Johnston
‘History’ • Initiation – 1991! • Expertise + experience • Grant application – funded by Chief Scientist Office • Differences ‘now’ • Co-applicants • MRC Framework for Complex Interventions • Power calculations • Randomisation
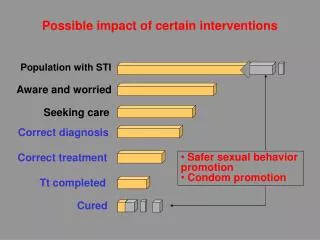
Background • MI: high frequency, disabling • Effects on families • Evidence that cardiac rehabilitation programmes effective • Questions • Timing • In patient vs outpatient? • Duration • Content • Emotional outcome • Recovery • Risk reduction • Involvement of partners • Partner emotional outcome • Effects on patient
A B Ewart et al
CARDIAC REHABILITATIONAND COUNSELLING TRIAL • Patients within a few days of myocardial infarction • Intervention using cognitive-behavioural technologies • increase information e.g. risk reduction • enhance perceived control • enhance coping with limitations and with emotions • Randomly allocated to intervention (in-patient or extended) or control • Outcome: changed - thoughts, emotions, activities Johnston et al., 1999
Research Questions After a first MI, do patients (and their partners) who receive an inpatient cardiac rehabilitation programme demonstrate: • Greater benefit than those receiving normal care? • Equal benefit to those receiving an extended programme? [benefit = knowledge, satisfaction with care, mood, disability]
Design • Patients following first MI and their partners • Randomised to: • Normal care • Inpatient CR • Extended CR up to 2 months following discharge • Followed up 2 weeks 2, 6 and 12 months • Blind assessment
Randomisation • Simple randomisation not possible • Randomisation of post CCU wards • Avoided confounding with wards and retain blind assessment by changing randomisation at variable intervals • Clearance periods
Cardiac Counselling and Rehabilitation Programme Delivery • [Normal care – no formal programme] • CR groups • within 3 days of admission • Inpatient up to 5 sessions [actual average 5.55, 3.69 hours] • Extended – up to 8 additional sessions [actual average 9.55, 8.43 hours] • Nurse counsellor – control for individual by having two • Manual • Non-judgemental counselling
Cardiac Counselling and Rehabilitation Programme Content • Aimed to enhance perceptions of control • Information • Action plans • Advice • Coping skills training • Relaxation • Leaflets and videos • Individual tailoring • menu
Menu • Explanation of heart attack • Emotional effects • Risk factors and their modification • Recovery period: resumption of activities • Investigations/treatment
Goal/target Monitoring Contract Planning Contingencies Grading task Skill enhancement Skill rehearsal Prompts Modelling Stress management Environmental changes Social pressure/support Persuasive communication Information re behaviour and outcome Personalised message Homework Personal experiments Experiential Evidence based techniques for changing behaviour
Inclusion criteria • All patients admitted to Ninewells CCU ie all from region • First MI (WHO criteria) • <70 years • Fluent in English • Able to participate • Informed consent (13 refused)
Participants • 117 randomly allocated • 10 withdrew • 7 died • Numbers in groups • Control 33 • Inpatient 38 • Extended 29 • No significant differences between 3 groups on demographic or clinical factors
Illustrative Baseline data[only Misconceptions significant – used as covariate]
Knowledge New questionnaire 19 statements Responses: true, false, don’t know Scores Correct (α = 0.68) Misconceptions (α = 0.57) Uncertainty (α = 0.74) Satisfaction with care 1 item ‘how satisfied do you feel generally about the advice that you received after your/your partner’s heart attack?’ Rated 1 to 10 1 = not at all satisfied 10 = extremely satisfied Outcomes – I: no standardised measures
partners patients Knowledge: Correct Significant group by time interaction: I and E > C at discharge and at 2 months Significant effects for Misconceptions and Uncertainty
Cardiac Rehabilitation and Counselling: Satisfaction Patients: significant main effect of group: significant interaction (E>I at 2mths) Partners: significant main effect of groups
Outcomes II: standard measures • MOOD: Hospital Anxiety and Depression Scale • DISABILITY/RESUMPTION OF NORMAL ACTIVITES: Functional Limitations Profile (UK version of Sickness Impact Profile)
Cardiac Rehabilitation and Counselling: Anxiety Significant interaction: I and E lower than C at 2 and 6 months
Cardiac Rehabilitation and Counselling: Anxiety Patients Partners Partners: significant interaction: I < C at discharge and 2 months; E< C at 2,6,12 months; E< I at 2 and 6 months
Cardiac Rehabilitation and Counselling: Depression Significant interaction: I < C at 2mths; E < C at 2, 6 and 12 mths
Cardiac Rehabilitation and Counselling: Depression patients partners Partners: significant interaction: I<C at 6mths; E<C at 2, 6 mths
Cardiac Rehabilitation and Counselling: Functional Limitations Profile total physical psychological Significant main effect of groups on all 3 measures: C>I, C>E
Discussion: Results • Results show benefits of CR • For both patients and partners • Some lasting to 12 months • Some extra benefit of extended programme – especially in partners • No differences between 2 counsellors • Did not have power to examine changes in risk factors
Discussion • Levels of anxiety in partners • Levels of satisfaction in partners • Results on anxiety similar to other studies • Differential effects on women and men • Lack of CR programmes in UK • Provided for highly selected patients • This intervention is implementable
Gender andActivity Limitations at follow-up control control Cardiac rehabilitation & counseling
Designing a Randomised Clinical Trial (RCT) to test if stress management reduces blood pressure in patients with hypertension (1986-1990) • Why do it? • High BP major risk factor for cardiovascular disease • Unclear how mildly raised BP should be treated • Some evidence that relaxation/stress management effective but previous studies poorly controlled • Unclear how well results generalised in previous studies
Main Design/measurement issues in this study • Control, stability of BP over time, & Generalisation • Control • Placebo control group or non-specific intervention i.e. has all the common components of the therapy but none of the specific (active) ones. • Exercise, flexibility training • Stability • Length of pre-treatment baseline (habituation). Multiple BP measures before start of treatment
Sample 7 Practices referred patients with 2/3 DBP 90-104 184 referred 3 month baseline (BP measured twice per day) 88 excluded (96 allocated to 2 treatments 32 BP too low 13 BP too high 6 too heavy, too high alcohol consumption 7 other illness 30 withdrew
Tightly controlled trial of stress management (like Patel), in approx. 100 mild hypertensives. Flexibility exercises used as control group. Long baseline (3 months), clinic ambulatory and stress testing of BP
Generalisation • Is BP measured clinically adequate for evaluating relaxation? • Ambulatory BP : Yes • Enduring effects of successful therapy on CV system (Left Ventricular Mass (LVM) : Yes • A clinical outcome: myocardial infarction (heart attack), death : No
Common issues in designing a RCT • Power • Analysis: “Intention to Treat” • Blind assessment • Cluster randomisation
Useful reference if contemplating conducting a RCT • Whole issue of Epidemiologic Reviews, 2002, 24, 1. • Edited by PW Lavori & JL Kelsey & covering • Design • Management • Analysis • Sample size • Ethics • More area specific topics
Assignment Rates of hospital induced infections are too high, possibly because the staff do not wash their hands. NHS Scotland proposes to introduce a new training package to improve staff hygiene but wish to evaluate it before requiring its use across the country. Design an RCT to evaluate the effectiveness of the package. 1 page single spaced. For Feb 13th