Download
1 / 38
380 likes | 595 Views
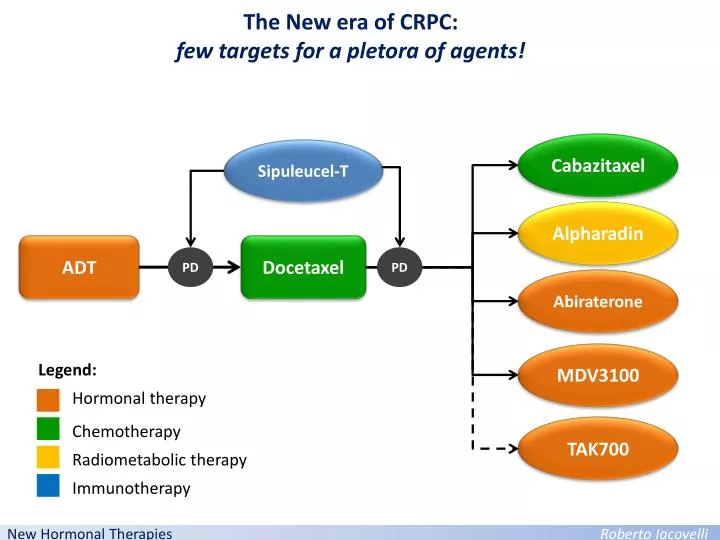
The New era of CRPC: few targets for a pletora of agents!. Cabazitaxel. Sipuleucel-T. Alpharadin. ADT. Docetaxel. PD. PD. Abiraterone. MDV3100. Legend:. Hormonal therapy. Chemotherapy. TAK700. Radiometabolic therapy. Immunotherapy. New Hormonal Therapies Roberto Iacovelli.

E N D
The New era of CRPC: few targets for a pletora of agents! Cabazitaxel Sipuleucel-T Alpharadin ADT Docetaxel PD PD Abiraterone MDV3100 Legend: Hormonal therapy Chemotherapy TAK700 Radiometabolic therapy Immunotherapy New HormonalTherapiesRoberto Iacovelli
Currentstrategies for androgeninibition in CRPC LH-RHa AR Abiraterone TAK700 Bicalutamide MDV3100 New HormonalTherapiesRoberto Iacovelli
Molecular basis for Androgen inibition in CRPC Hormon sensitive PCa Negative control CRPC cells Il recettore per l’androgeno (AR) è espresso (RNA) sianeitumorisensibilicheresistentiallacastrazione Dillard et al. Mol Cell Endocrinol. 2008 New HormonalTherapiesRoberto Iacovelli
Molecularbasis for Androgeninibition in CRPC H&E BP=benign prostate tissue; CP=Prostate cancer; METS=castration-resistant metastatic tumor AR staining Metastasis of CRPC PSA staining Montgomery et al. Cancer Res 2008;68:4447-4454. New HormonalTherapiesRoberto Iacovelli
Molecularbasis for Androgeninibition in CRPC Hormon sensitive PCa Normal epithelium CRPC cells CRPC cells Control CYP17 is expressed in CRPC cells. CYP17 is not expressed in hormone sensitive cells. CYP17 is not expressed in normal prostatic epithelium New HormonalTherapiesRoberto Iacovelli
Molecular basis for Androgen inibition in CRPC Expression of steroidogenic enzyme transcripts in primary and metastatic prostate tumors BP=benign prostate tissue; CP=Prostate cancer; METS=castration-resistant metastatic tumor Montgomery et al. Cancer Res 2008;68:4447-4454. New HormonalTherapiesRoberto Iacovelli
Molecularbasis for Androgeninibition in CRPC CRPC cell acquires the ability to product itself testosterone from cholesterol by CYP17 New HormonalTherapiesRoberto Iacovelli
Molecularbasis for Androgeninibition in CRPC Testosterone AR AR CYP17 Hormone sensitive PCa cell CRPC cell ENDOCRINE Pathway PARACRINE Pathway AUTOCRINE Pathway Increase of malignancy New HormonalTherapiesRoberto Iacovelli
Molecularbasis for Androgeninibition in CRPC Efstathiou E. Clin Cancer Res 2010;16:1100-1107 New HormonalTherapiesRoberto Iacovelli
Targeting CYP17 CYP17 CYP17 inhibitor Iacovelli et al. Anti-Cancer Drugs 2011. New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate A new molecule who meet oncological need in prostate cancer: Proved efficacy in post docetaxel patients Increase the time to chemotherapy Pain PSA Progression Tumor/Bone Progression ECOG PS Decline Death Baseline Chemotherapy Increase OS 24-48 months Adapted from Halabi S. J Clin Oncol. 2009;27: 2766-2771 Ryan et al. ASCO 2012; Abstract LBA4518 (Oral Presentation) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate: proves of efficacy Abiraterone acetate CRPC chemo- naïve CRPC TXT pretreated 1 phase III Trial 1 phase III Trial 3 phase II Trials 1 phase I Trial Iacovelli et al. Anti-Cancer Drugs 2011. New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate CRPC TXT pretreated • Abiraterone acetate: selective inhibitor of androgen biosynthesis that blocks CYP17 activity • Primary endpoint: OS Randomized 2:1 Abiraterone acetate 1000 mg/day + Prednisone 5 mg BID (n = 797) Patients with mCRPC progressing after 1-2 chemotherapy regimens, 1 of which contained docetaxel (N = 1195) Stratified by ECOG PS, worst pain over previous 24 hrs, previous chemotherapy, type of progression Placebo + Prednisone 5 mg BID (n = 398) Study stopped at planned interim analysis at 534 events because OS improvement crossed predetermined stopping boundary de Bono JS et al. N Engl J Med. 2011;364:1995-2005. New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate CRPC TXT pretreated OS PFS New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate AdverseEvents *Most frequent cardiac disorders were tachycardia and atrial fibrillation. de Bono JS, et al. N Eng J Med. 2011;364:1995-2005. Scher HI, et al. ASCO GU 2011. Abstract 4. New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate CRPC chemo- naïve RANDOMIZED 1:1 Efficacy end points Patients AA 1000 mg daily Prednisone 5 mg BID (Actual n = 546) • Co-Primary: • rPFS by central review • OS • Secondary: • Time to opiate use (cancer-related pain) • Time to initiation of chemotherapy • Time to ECOG-PS deterioration • TTPP • Progressive chemo-naïve mCRPC patients(Planned N = 1088) • Asymptomatic or mildly symptomatic Placebo daily Prednisone 5 mg BID (Actual n = 542) • Phase 3 multicenter, randomized, double-blind, placebo-controlled study conducted at 151 sites in 12 countries; USA, Europe, Australia, Canada • Stratification by ECOG performance status 0 vs. 1 Ryan et al. ASCO 2012; Abstract LBA4518 (Oral Presentation) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate CRPC chemo- naïve Treatment Arms Evenly Matched Ryan et al. ASCO 2012; Abstract LBA4518 (Oral Presentation) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate: PFS CRPC chemo- naïve 100 80 60 Progression-Free (%) 40 20 AA + P PL + P 0 3 6 9 12 15 18 0 Time to Progression or Death (Months) AA PL 546 542 489 400 340 204 164 90 46 30 12 3 0 0 Ryan et al. ASCO 2012; Abstract LBA4518 (Oral Presentation) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate: OS CRPC chemo- naïve 100 80 60 Survival (%) 40 20 AA + P PL + P 0 3 6 9 12 15 18 21 24 27 30 33 0 Time to Death (Months) 546 542 538 534 524 509 503 493 482 465 452 437 412 387 258 237 120 106 27 25 0 2 0 0 AA PL Ryan et al. ASCO 2012; Abstract LBA4518 (Oral Presentation) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate: secondary end-points CRPC chemo- naïve Note: All secondary end points remain significant after adjusting for multiplicity testing Patient Reported Outcomes favored AA +P vs. Placebo +P Full data to be reported Ryan et al. ASCO 2012; Abstract LBA4518 (Oral Presentation) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate: Subsequent Therapy Was Common CRPC chemo- naïve Despite 16% of patients did not receive subsequent therapy compared to placebo, AA increase OS! *Prior to unblinding (e.g. not per protocol) New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate AdverseEvents *Most frequent cardiac disorders were tachycardia and atrial fibrillation. de Bono JS, et al. N Eng J Med. 2011;364:1995-2005. Scher HI, et al. ASCO GU 2011. Abstract 4. New HormonalTherapiesRoberto Iacovelli
Abiraterone acetate: Correct timing • AR stimolato anche aspecificamente • sintesi enzimi produzione T • AR ipersensibile o iperespresso • sintesi di TUTTI gli enzimi produzione T • AR ipersensibile o iperespresso • sintesi di alcuni enzimi produzione T • AR normale • No enzimi produzione T New HormonalTherapiesRoberto Iacovelli
Cytoreduction and androgensignalingmodulationby abiraterone acetate (AA) plus leuprolide acetate (LHRHa) versus LHRHa in localizedhigh-risk prostate cancer (PCa): Preliminaryresultsof a randomizedpreoperativestudy. RANDOMIZED 2:1 SURGERY Efficacy end points Patients AA 1000 mg daily Prednisone 5 mg BID + LHRHa for 12 wks • Co-Primary: • difference in down staging (≤ ypT2) • safety • Secondary: • difference in androgen biosynthesis, androgen signaling, proliferation apoptosis and candidate treatment resistance pathways. • high risk PCa (clinical stage ≥T1c and biopsy Gleason score ≥8, or ≥T2b, Gleason ≥ 7 and PSA > 10ng/ml). LHRHa For 12 wks Results:
Abiraterone acetate 35% of patients had PD as best response a 3 mos with Abiraterone. What is the mechanism of resistance? New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) Antitumor activity of Enzalutamide in Phase I/II study Activity seems to be independent of previous chemotherapy Scher HI, et al. Lancet 2010;375:1437 New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) The AFFIRM Trial Design Primary End-Point: OS Stratification variables: ECOG-PS, meand BPI (<4, ≥4) Statistical design: power 90% to detect a 24% reduction in mortality (target HR= 0.76). New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) Baseline patient demographics: New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) RESULTS: The AFFIRM study was halted and unblinded after the interim analysis (520 events). Target 0.76! New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) RESULTS: PSA response rate, PSA-PFS and Time To First Skeletal Event HR denosumab vs placebo 0.84!* *Smith MR et al. Lancet 2012 New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) RESULTS: Survival benefit across all subgroups New HormonalTherapiesRoberto Iacovelli
Enzalutamide (MDV3100) RESULTS: Safety New HormonalTherapiesRoberto Iacovelli
Conclusions Androgen pathways is the driver of tumor progression of prostate cancer. Resistance to LHRHa don’t mean resistance to all hormonal strategies. CYP17 and AR are the main targets of new hormonal therapies The sequential use of these agents may be feasible but not proven in large prospective trial. Precocious use of new agents seems to be more active.
Q&A Durante il trattamento l’analogo deve essere proseguito? È Possibile rinunciare al trattamento con prednisone? In controllo con placebo o Prednisone è idoneo? New HormonalTherapiesRoberto Iacovelli
Is prednisone an active control for CRPC? The AFFIRM study reported a PSA decline >50% in 2% of patients treated with placebo alone! New HormonalTherapiesRoberto Iacovelli