Download
1 / 22

E N D
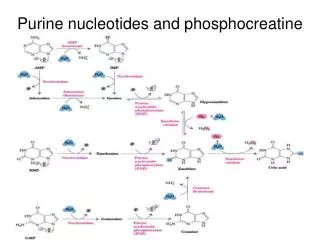
M.Prasad Naidu MSc Medical Biochemistry, Ph.D,. Purine Catabolism and its disorders
Catabolism of purines : FAD, Molybdenum,iron
The end product of purine catabolism is uric acid • in humans. • Uric acid is degraded into allantoic acid and finally to ammonia in animals other than man. • Uric acid is 2,6,8 –trioxy purine. • It acts as antioxidant by converting itself into allantoin.
Uric acid • Normal serum concentration: 3 to 7 mg /dl in males • 2 to 5 mg/dl in females • Miscible pool– the quantity of uric acid present in • body water. It is on average of 1130mg • Daily turnover: 500 to 600 mg synthesized • 400 to 600 mg/day excreted • Uric acid isclearedby both • glomerular filtration and • tubular secretion.
Hyperuricemia and gout: • Hyperuricemia – increased serum uric acid levels. • Goutis a metabolic disorder of purine catabolism, • resulting in overproduction of uric acid. • At physiological pH , uric acid is more soluble than urates.
In hyperuricemia ,serum urate levels exceed • solubility limit, leading to formation of crystals and • get deposited in joints.The deposits are called tophi. • Tophi cause inflammation of joints resulting in painful • acute gouty arthritis, that can progress to chronic • gouty arthritis leading to urolithiasis and renal damage.
Clinical features: • Manifestations are due to the low solubility of uric acid in water. • Typical gouty arthritis affects first • metatarsophalangeal joint.(GREAT TOE). • Attacks are precipitated by alcohol intake. • Often patient have few drinks , go to sleep • symptomless , but are awakened during early • hours by severe joint pains. • Synovial fluid shows birefringent crystalsunder polar microscope is diagnostic.
Types of gout : • 1.Primary gout:a) metabolic b) renal • Metabolic Causes : • Abnormal enzyme - PRPP --- glutamylamidotransferase is active but not sensitive to feedback control. • Variant form of PRPP synthetase- not subject to allosteric control. • Deficiency of enzymes of salvage pathway –HGPRT deficiency leading to Lesch-Nyhan syndrome. • b) Renal causes: due to failure in uric acid excretion.
2. Secondary gout: a)Overproduction of uircacid – due to enhanced turn over rate of nucleic acids i) Increased tissue turn over due to psoriasis. ii) rapidly growing malignant tissues-leukemias. ii)Increased tissue break down – after treatment for large tumour masses. (with radiation,chemotherapy)
b)Reduced excretion of uric acid • Increased alcohol consumption leads to lactic -acidosis. Lactic acid inhibits uric acid excretion. • Thiazide diuretics inhibits tubular secretion of uric acid. • Renal failure. • c) OTHERS • VONGIERKE’S DISEASE • Elevated glutathione reductase
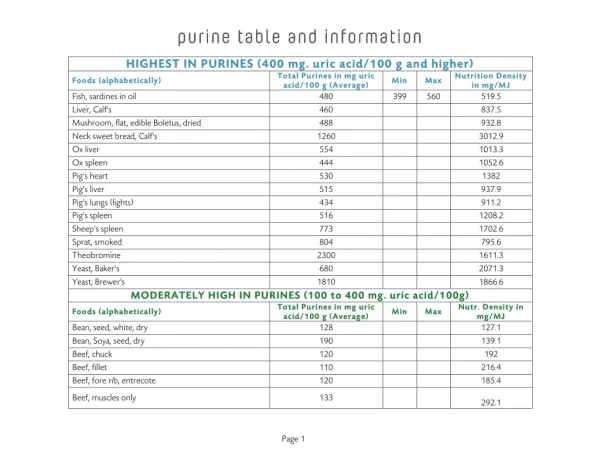
Treatment: • Low intake of purine diet • Restrict alcohol • Drugs: • 1.uricosuric drugs – probenecid,salicylates,halofenate • 2. enzyme inhibitors – allopurinol
Action of allopurinol: Allopurinol alloxanthine xanthine oxidase inhibits Xanthine and hypoxanthine are more soluble and excreted easily.
Palliative treatment : • Anti-inflammatory drugs : • Colchicine is used . • Others include indomethacin , ibuprofen. • Steroids also used.
Lesch-Nyhan syndrome: Inheritance pattern -- X-linked recessive Enzyme defect(salvage pathway) -- hypoxanthine guanine phoshoribosyl transferase (HGPRT) Rate of salvage pathway decreases Accumulation of intracellular PRPP and decrease in GMP and IMP ,the inhibitory nucleotides Increased production and degradation of purine nucleotides.
Features: • Only males are affected, as structural gene for HGPRT is on X- chromosome. • Characterised by excess formation of uric acid. • Nephrolithiasis • Selfmutilation • Neurological abnormalities like mental -retardation, aggressive behavior , learning disabilities occur. • Neurological symptoms may be due to dependence of brainon the salvage pathway.
Adenosine deaminase deficiency and purine- nucleoside phosphorylase deficeincy: Both are Inherited as autosomal recessive. Deficeincy ADA purine nucleoside phosphorylase Both T and T-cells affected , B-cells affected. B -cells are normal.
Immune dysfunction appear to result from • accumulation of dGTP and dATP • . • These allosterically inhibits ribonucleotide- • reductase,thereby depletes cells of DNA • precursors, particularly dCTP. • HYPOURICEMIA.
VONGIERKE’S DISEASE : Glucose-6-phophatase
Pseudogout : • Serum uric acid level normal. • Symptoms as seen in gout. • But it is characterised by deposition of calcium – • pyrophosphate crystals.
Hypouricemia : • Xanthine oxidase deficiency, either genetic or due to • severe liver damage. • Patients exhibit xanthinuria and xanthine lithiasis.