Download
1 / 59
670 likes | 1.37k Views
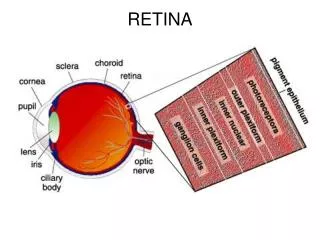
retina. Švehlíková G. LF UPJS v Košiciach Prednosta: prof. MUDr. Juhás T., DrSc. retina. Anatomy. Retina. 1. Retinal vascular diseases – AH, CRAO, CRVO, Diabetic retinopathy , 2. Infections

E N D
retina Švehlíková G. LF UPJS v Košiciach Prednosta: prof. MUDr. Juhás T., DrSc
Retina • 1. Retinalvasculardiseases – AH, CRAO, CRVO, Diabeticretinopathy, • 2. Infections • 3. AquiredMaculardisorders – ARMD, Centralserouschorioretinopathy, macularsurfacedisorders • 4. Hereditaryfundusdystrophies • 5. RetinalDetachment • 5. Retinaltumors
Ffluoresceinangiography • Flourescein angiography - is a test to examine blood vessels in the retina and choroid Normal FA
AH – hypertensivearteriolopathy, retinopathy • Prolongedhypertenzion • Funduspicture – • vasoconstriction – arteriolarnarrowing • leakage – abnormalvascularperemability – hemorages, exudates, retinaloedema • arteriolosclerosis – thickeningofthevesselwall – changesat AV crossings
Centralret. arteryocclusion Causes Embolism – fromtheheart carotid a. disease ( cholesterol, fibrinoplatelet, calcific ) Vaso-obliteration – atherosclerosis, periarteritis – asociatedwithsystem. vascl., haematolog. disorders
Centralret. arteryocclusion • Presentation • Acutelossofvision • Signs • retina – white, fovea in contrasred • arterioles and venules – narrow • central, branch • Treatment • Ocularmassage, IOP ↓,
Centralret. veinocclusion Predisposingfactors Systemic – age, systemichypertension, diabetes ( veiniscompressed by thethickedartery), bloodhyperviscosity Ocular - ↑IOP, hypermetropia, congenitalabnormal.
Centralret. veinocclusion • central, branch • Presentation • -moderatelossofvisulaacuity • Signs • tortuosity and dilatationofretinalvein, • hemorrhages • cotton-woolspots • Opticdiscoedema • Complication- CME, neovascularisation
Diabeticretinopathy Prevalence IDD 40%, NIDD 20% Microangiopathy – reduction in thenumberofpericytes – distensionofcapillarywalls, breackdownoftheblood- retinalbarier – leakage Theconsequenceofretinalnon-perfusionisretinalischaemia - hypoxia Hypoxia – causes A-V shunts and neovascularisation
Diabeticretinopathy Nonproliferative DR Intraretinal HE, hardexudates, oedema
Diabeticretinopathy Neovascularisation Th – laser photocoagulation Complication- HE, tractionalretinaldetachment Proliferative DR
Diabeticretinopathy Nonproliferative DR Proliferative DR
Proliferative DR fluoresceinangiography NVE NVE FA
The most important causes of retinal vasculitis • Idiopathic • Behçet’s disease • Multiple sclerosis • Lupus erythematosus • Wegener’s granulomatosis • Polyarteritisnodosa • Horton’s arteritis • Sarcoidosis • Tuberculosis • Borreliosis (Lyme disease) • Listeriosis • Brucellosis • Syphilis • Viruses
Age-relatedmaculardegenerationAMD Types – Atrophic- non-exudative– slowlyprogresive, 90% Exudative – wetform – detachmentof RPE, choroidalneovascularisation
Atrophic, dry, nonexudative AMD The most common type, 90% Slowlyprogresiveatrophyofthe RPE and photoreceptors Presentation – gradualmild- to – moderataimpairmentofvision over severalmonth or years. Drusen Depositionofabnormalmaterial in Bruchmembrane
The Amsler grid is used to detect small irregularities in the central 20 degrees of the field of vision. • Is a quick and simple test that patients are asked to use to monitor changes in their vision
OCT • Optical Coherence Tomography (OCT) is a new imaging technique that provides high resolution and cross-sectional images of the eye • analogous to ultrasound, but instead of usingof acoustic waves (as in ultrasound), it uses light to achieve micrometer axial resolution. • the axial resolution of OCT in retinal tissue is about 1-15 µm, which is 10 to 100 times better than ultrasound or MRI • anatomic layers within the retina can be differentiated and retinal thickness can be measured.
Late – geographicatrophy Atrophic AMD Early – drusen
Exudative AMD • Lesscommon, visionlossfastwithinfewweeks • In isolation or in associationwithatrophic AMD • Exudativedetachmentofthe RPE • Choroidalneovascularisation • growfromthechoriocapillaristhroughdefects in Bruchmembr. Intothesub- RPE space
Disciformscar AMD exudativeform Choroidalneovascularization
Centralserousretinopathy Idiopatic, self-limiteddiseaseofyoung or midle-agedadultmales usualyunilateral, localizeddetachmentofthesensoryret. Presentation suddenblurredvision in oneeye, associatedwithmetamorphopsia FAG – breakdownoftheblood-retinalbarrierwhitchallowsthepassageoffluoresceinintosubretinalspace Prognosis 80% spontaneousresolution, normalvisionwithin 1-6 month 20% resolvewithin 12 month Prolongeddetachment or recurrentattacks – permanentimpairmentofvisualfunction
macularsurfacedisorders • Idiopathicmacular hole • Macularpucker
Idiopathicmacular hole • Pathogenesis: • focalcontractionoftheperifovealvitreouscortex and itsseparationfromretinalsurface • Signs • round hole surrounded by o hakoofretinaldetachment • VA ↓ • Th: PPV • results : 60%
Macular Pucker • abnormal scar tissue membrane - epiretinal membrane, ERM- which grows over the surface to the macula • this causes wrinkling of the macula and subsequent distortion of central vision - metamorphopsia • these ERMs may grow as a result of aging, diabetes, trauma, inflammation, or previous eye surgery
Hereditarydegenerations • Photorectordystrophies - Retinitispigmetosa • Dystrophiesof RPE - fundusflavimaculatus • Choroidaldystrof. - choroideremia, Gyrateatrophy • Albinism
Retinitispigmentosa • groupofhereditarydisorders • – progressivelossofphotoreceptors • diffuse, usuallybilat. , symetrical • cones, rods - predominant • Presentation – defectivedarkadaptation ( nightblindes – nyctalopia)
Myopicretinopathy • Degenerativemyopia • progresiveelongationoftheglobeisfollowed by degenerativechanges in theretina and choroid • Signs • - islandsofchorioretinalatrophy • atrophyaroundtheopticdisc • Macula – breaks in Bruchmemb., neovascularisation, haemorarrhage • posteriorstaphyloma, peripheraldegeneration
Retinaldetachment • separationofthesensoryretinafromthe pigment epitelium • Rhegmatogenous – retinal break • Non-rhegmatogenes - tractional • exudative
Rhegmatogenousretinaldetachment • Affects 1/10 000 • rhegma means break in greek • It occurs in patients with • history of previous trauma to the eye • myopy • peripheral retinal degenerations like lattice degeneration
Posterior Vitreous Detachment (PVD) • In healthy eyes of young patients, the vitreous is a clear gel that fills the vitreous cavity • vitreous consists mostly of water (99 %) as well as hyaluronic acid and a meshwork of fine collagen fibrils • important area is the vitreous base - 3-4-mm-wide circumferential zone of vitreous • in the vitreous base, the collagen fibers are firmly attached to the underlying peripheral retina • other areas of firm vitreous attachment are at • the optic disc • along the major vascular arcades • the edges of retinal scars • in areas of vitreoretinal degenerations
Posterior Vitreous Detachment (PVD) • With age the vitreous begins to liquefy and shrink • this normal process usually starts between 45 and 55 years of age • PVD is the separation of the vitreous from the posterior portion of the retina • prevalence of PVD increases with age, with axial length, and following cataract surgery and trauma • Clinical Features:patients with acute PVD experience flashes of light –photopsia - and/or "floaters" • flashes represent retinal stimulation from vitreous traction • floaters are shadows
Posterior Vitreous Detachment (PVD) • PVD might tear the retina at areas where the vitreous is firmly attached • when a piece of the retina is torn free, the remaining tear is called operculated tear • when the torn retina remains adherent , we have a flap or Horseshoe tear • flap tears are more likely to progress into retinal detachment than operculated tears, because of the continuing vitreal traction on the retinal flap • ManagementThe fundus should be carefully examined to rule out retinal tears • the great majority of PVDs do not cause a retinal tear
peripheral retinal degenerations • Benign • Predisposingperif. ret. degenerat.
peripheral retinal degenerations benign predisposing
peripheral retinal degenerations Benign snowflakes Predisposing snailtrack
Rhegmatogenousretinaldetachment • can occur once there is a retinal break • liquid vitreous passes through the break and goes under the retina • retina will then start to detach from the underlying tissue • most tears occur in the peripheral retina → the detachment will first cause loss of a portion of the side vision • this can be seen as a curtain or dark shadow involving the peripheral vision. As the detachment extends towards the macula, the shadow will also enlarge. Central vision will be lost if the macula detaches
Traction Retinal Detachment • Definition:The retina is pulled into the vitreous cavity by transvitreal traction • Etiology: Diabetic Retinopathy, PVR, old penetrating injuries... • Clinical Features: The detached retina is smooth, immobile, and concave toward the pupil. No breaks are usually found on ophthalmoscopy. • Management:Vitrectomy, with release of vitreous tractions is required
ExudativeRetinalDetachment • Definition:Theresultofcollectionof fluid beneathanintactsensoryretina. • Etiology:Choroidalneoplasm (e.gmelanoma), chorioretinalinflammatorydiseases, malignanthypertension (as in toxemiaofpregnancy), hemorrhagefrom a subretinalneo-vascularmembrane( as in AMD), systemicvascular and inflammatorydiseases. • ClinicalFeatures:smooth, transparent retinalelevation • no retinalbreaks nor pigment clumps or redbloodcells in thevitreous are identified • Management - treattheunderlyingconditionifpossible.
Management Each procedure requires location of the tear and treating the retina around its edges by cryotherapy or laser in order to create firm adhesions between the sensory retina and the RPE layer and preventing detachmnent. • Pneumatic retinopexy is best done for superior breaks • The gas bubble will expand and being lighter than the ocular fluids, will migrate upward to tamponade superior breaks • Positioning - if the break is in the posterior pole (close to the macula), the patient should remain face down. • If the break was in the right temporal retina, he should lie flat on his left side. • Positioning should be applied for the first 2 weeks..
Management • 1. Scleral Buckle: • silicone explant- over the sclera 360 degrees - in order to indent the sclera and make it apposed to the underlying detached retina. • 2. Pneumatic Retinopexy: - Intra-ocular injection of gas ( air or expandable gas) in order to tamponade the retinal detachment and break while the choroidal adhesions form • 3. Vitrectomy with silicone oil