Download
1 / 20
270 likes | 1.11k Views
Diagnosis of tuberculous pleurisy. Acute onset on high risk person (TB contact, radiological suggestive lesions) Fever in young adults (the elderly-without fever) Chest pain (often axillary) Dry cough triggered by changing of position

E N D
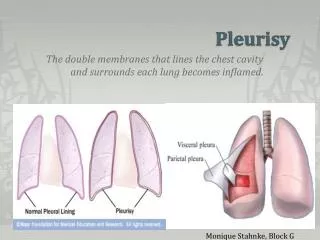
Acute onset on high risk person (TB contact, radiological suggestive lesions) Fever in young adults (the elderly-without fever) Chest pain (often axillary) Dry cough triggered by changing of position Sometimesimportant dyspnea – depending on the volume of pleural effusion Physical signs: Dullness to percussion, and decreased breath sounds and voice vibrations The affected hemithorax - the respiratory movements are reduced Bulging of the affected hemithorax - inpatients with large pleural effusion Egophony (E-to-A change) Pleural friction rub Clinical diagnosis
Paraclinical diagnosis –RADIOLOGICAL EXAMINATION - Typical image of right basal pleurisy – opacity with mild intensity, with upper limit superior concave, in meniscus
Meniscus opacity with concave superior limit - upwards and inwards in two thirds lower left hemithorax
MASIVE PLEURISY- homogeneous opacity in the right hemithorax; Mediastinal shift away from the effusion: This is observed with effusions of greater than 1000 mL. (opposed to the appearance of atelectasis)
Radiological changes • Ascension of the hemidiaphragm on the affected side • The diaphragmatic dome is located more laterally than it should (the third side of the diaphragm and not its center) • Costo-diaphragmatic sinus is shorter • On the left side is an opacity, triangular shaped given by the retro-cardiac and para-mediastinal accumulation of liquid • On the profile radiography is described a net opacification in the posterior costo-phrenic sinus, even though the front side radiographs appear normal
Intradermal TB test (tuberculine skin test) • It is mandatory for all patients with exudative pleurisy • May be negative in the acute phase of fluid formation • If the patient is not allergic, the test will be positive in the next two months • Negative TST does not exclude TB pleurisy • A positive TST in case of exudative pleurisy, after a careful investigation, requires tuberculostatic treatment to be started
Morphopathological examination • Macroscopic aspects - serous fluid – milliary gray-white granulations - clamps and adherent - fibrin deposits - inflammatory response - rarely hemorrhagic reaction - neo membranes • Microscopic aspects – bare pleura - hyperemia under mesothelium layer - fibrin deposits – gigantepithelioid follicles ± center necrosis - caseting necrosis • Evolution - restitutio ad integrum - granulation tissue + fibrin -> pachipleuritis - adherent -> pleural fibrosis -> bronchiectasis
Pleural fluid examination • Appearance is most commonly serous > 90% of cases • Rarely hemorrhagic • Very rarely purulent fluid (TB pleural empyema)
Diagnostic approach to pleural effusions Etiology unknown Etiology probable (e.g. cardiac/renal) THORACENTESIS Persistencewith therapy Improvementwith therapy Colour? Protein? Cells? Others? • Positive finding of • malignant cells • bacteria, fungus etc. • other specific parameter, e.g. amylase (>serum)
The initial diagnostic consideration is distinguishing transudates from exudates. • Although a number of chemical tests have been proposed to differentiate pleural fluid transudates from exudates, the tests first proposed by Light et al have become the criterion standards.
The fluid is considered an exudate if any of the following apply: • Ratio of pleural fluid to serum protein greater than 0.5 • Ratio of pleural fluid to serum lactate dehydrogenase (LDH) greater than 0.6 • Pleural fluid LDH greater than two thirds of the upper limits of normal serum value
Biochemistry Pleural protein > 30 g/l (exudate) Pleural glucose < 0.6 g/l ADA (adenosine desaminase)> 30 (45) UI/l Pleural lysozyme/serum lysozyme > 2 Cytology Lymphocytes > 80% PMN increased in the early stages Repair lesions - increased eosinophils Pleural T lymphocytes > serum T lymphocites The absence or low number of mesothelial cells TB pleurisy
Bacteriological examination • Can provide etiological certainty • Microscopically and culture are positive in only a 5-10% cases • Pleural biopsy associated withseeding of a fragment of tissue on specific media culture for BK - increases to 50-80% the detection of TB pleurisy
Diagnostic approach to pleural effusions Etiology probable (e.g. cardiac/renal) Etiology unknown THORACENTESIS Improvementwith therapy Persistencewith therapy Colour? Protein? Cells? Others? Etiology unknown • Positive finding of • malignant cells • bacteria, fungus etc. • other specific parameter, e.g. amylase (>serum) CLOSED PLEURAL BIOPSY Etiology unknown Histological finding of malignancy ortuberculosis MEDICALTHORACOSCOPY Follow-up Etiology unknown (<10%) In single cases surgical biopsy
Positive diagnosis • Positive diagnosis of tuberculous pleurisy is based primarily on bacteriological and histological confirmation, together able to provide diagnosis in over 85% of cases. • Most important arguments for the etiology of TB can be summarized:- age under 35-40 years;- serous fluid - lymphocyte predominant;- pleural fluid protein above 30 g/l and pleural glucose under 0.60 g/l;- a positive TST or TST becomes positive after 4-6 weeks of tuberculostatic treatment;- increased ADA in pleural fluid;- report of pleural lysozyme/serum lysozyme than 2;- healing with scars;- favorable evolution under tuberculostatics treatment
Diagnostic approach to pleural effusions thoracentesis etiology ? closed pleural biopsy etiology ? medical thoracoscopy etiology ? surgicalbiopsy follow-up
REFERENCES http://webcache.googleusercontent.com/search?q=cache:T22sqis_JwAJ:emedicine.medscape.com/article/299959-overview+light+criteria+to+pleuresy&cd=1&hl=ro&ct=clnk&gl=ro