Download
1 / 52
520 likes | 618 Views
Drug Development in HIV. Michael Zaiac New Product Development 25/11/05. Contents. Background-Setting the scene Co receptors and HIV Co-receptor tropism Co-receptors as targets Philanthropy Summary. No Sign of Pandemic Abating. Issues No vaccines on horizon

E N D
Drug Development in HIV Michael Zaiac New Product Development 25/11/05
Contents • Background-Setting the scene • Co receptors and HIV • Co-receptor tropism • Co-receptors as targets • Philanthropy • Summary
No Sign of Pandemic Abating Issues • No vaccines on horizon • Resistance to ARV drugs increasing • Western World - re-invigorate public health campaigns - new ARV to address resistance & compliance • Developing World - ARV to break infection cycle - healthcare infrastructure & public education - economic stability - global political leadership
Eastern Europe & Central Asia 1.4 million 210,00060,000 North America and Western/Central Europe 1.6 million 64,000 23,000 North Africa & Middle East 540,000 92,00028,000 Asia 8.2 million 1.2 million540,000 Caribbean 440,000 53,000 36,000 Sub-Saharan Africa 25.4 million 3.1 million2.3 million Latin America 1.7 million 240,00095,000 Oceania 35,000 5000700 Total living cases: 39.4 million New cases, 2004: 4.9 million AIDS Deaths, 2004: 3.1 million Estimated Number of People Living With HIV, by Region in 2004 UNAIDS/WHO, 2005
Goals of Antiretroviral Treatment 1. Prevention of progressive immunodeficiency;potential maintenance or reconstruction of a normal immune system 2. Control of viral replication and mutation; reduceviral burden Delayed progression to AIDS and prolongation of life Decreased risk of selection of resistant virus
Anti-Retroviral Therapy • Explosion in HIV research since 1980 & AZT in 1987 • But…HIV challenging target - obligate parasite, so few viral targets - high mutation rate & genetic plasticity • > 20 approved agents but only 4 targets • Combination therapy (at least 3 agents) = HAART introduced in 1995 - reduce propensity to resistance
Genetic Plasticity • 109 new virions produced daily • One mutation during every replication cycle per cellular genome • Genetic plasticity enables HIV to: - evade immune system - develop resistance to ARV - produce mutants with different ‘fitness’ • Multiple strains co-exist & are archived in patients’ immune cells
Emergence of HIV Resistance Total plasma HIV RNA Wild-type (WT) HIV RNA Mutant HIV RNA Plasma HIV RNA Time Receiving Treatment Havlir. Ann Int Med 1996:124:984.
Class Drug Nucleoside/tide Reverse Transcriptase Inhibitors Zidovudine, Zalcitabine, Didanosine/EC, Stavudine/XR, Combivir, Trizivir, Lamivudine, Abacavir, Tenofovir Non-Nucleoside Reverse Transcriptase Inhibitors Efavirenz, Delavirdine, Nevirapine Enfuvirtide Fusion Inhibitors Protease Inhibitors Saquinavir, Indinavir, Ritonavir, Nelfinavir, Amprenavir, Lopinavir/Ritonavir, Atazanavir Approved ARV Agents
Problems with HAART • HAART = HIV chronic disease & saves lives • But… most agents designed for acute disease • HAART has considerable drawbacks: - toxicity & side effects - drug interactions - high pill burden & inconvenient dosing • Tox. & inconvenient dosing reduce compliance • Resistance emerges within 6 months to 5 years - up to 27% of newly diagnosed HIV is resistant
= compliance & durability Requirements on HIV medicines Ideal features of an antiretroviral agent: - low dose - convenient regimen - better toleration - non cross resistant - new mechanisms & targets - low COG
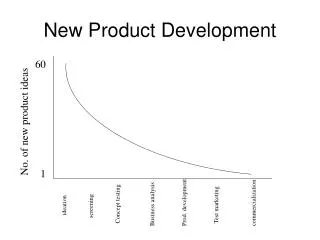
Attrition on the R&D Process 1 Medicine
Years 0 1 2 3 4 5 6 7 8 9 Candidate attrition 25 animal toxicity, chemical stability, superior compound human PK, tolerability, formulation 12 No. candidates Efficacy, safety, differentiation, Dose, c.o.g. long-term safety non-approval 4 0 Preclin. Phase I Phase II Phase III Registration
0 1 2 3 4 5 6 7 8 9 10 New medicine development Medicine Development Costs Time/Cost of Medicine Development Launch £450 million File 500 400 £280 million Phase III 300 £200 million Cumulative costs £M Phase I 200 Phase II £70 million 100 £30 million 0 Years
CCR5 and CXCR4 Co-Receptors:HIV Binding and Entry CD4 CXCR4 CCR5 T-Cell Surface
HIV-1 Envelope Glycoproteins HIV-1 gp41 gp120 HIV-1 Envelope Glycoprotein CD4 CCR5 T-Cell Surface
Binding of the gp120 Subunit of the HIV-1 Envelope Glycoprotein to CD4 HIV-1 gp41 gp120 CD4 CCR5 T-Cell Surface
Conformational Change Exposes theCo-Receptor Binding Site in gp120 HIV-1 gp41 gp120 CD4 CCR5 T-Cell Surface
Conformational Change Allows gp120 to Bind to the Co-Receptor HIV-1 gp41 gp120 CD4 CCR5 T-Cell Surface
Fusion of HIV and T-Cell Membranes HIV-1 RNA HIV-1 HIV-1 Nucleocapsid T-Cell Surface
HIV-1 Tropism Assays:MT-2 Cell Assay • Indirect measure of co-receptor use • Depends on the presence of X4 or R5/X4 isolates • Uses viral stocks from stimulated patient lymphocytes • Results are reader dependent and involve the interpretation of typical cytopathic changes • Limitations • HIV derived from stimulated lymphocytes may differ from that of plasma virus • Qualitative nature of the assay result • Detection of CXCR4 only Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126. DAIDS Virology Manual for HIV Laboratories. 1997. Publication NIH-97-3828. U.S. Department of Health and Human Services, Washington, DC.
MT2 cell assay Syncytium Formation in MT-2 Cells • Prior to the discovery of the role that CCR5 and CXCR4 play in viral entry, viruses were characterized by ability to infect T-cells and cause syncytium formation • MT-2 cell lines were used • MT-2 cells express only CXCR4 • Syncytium inducing (SI) • Changed to CXCR4-using virus • Non-syncytium inducing (NSI) • Changed to CCR5-using virus Schuitemaker H, et al. J Virol. 1991;65:356-363. Japour AJ. J Clin Microbiol. 1994;32:2291-2294.
HIV-1 Tropism Assays:Recombinant Phenotypic Assays • Direct measure of co-receptor use • Infect engineered cell lines to determine co-receptor utilization • Obtained by RT-PCR from patient plasma sample • Virus stocks pseudotyped with envelope sequences derived from patient plasma samples • Limitations • >500 copies/mL • May fail to detect X4 when X4 virus constitutes <10% of the viral population • Sequence variation may result in assay failure Coakley E, et al. Curr Opin Infect Dis. 2005;18:9-15.
CD4 + CXCR4 + HIV env expression vector HIV genomic luc vector + Infection Transfection Pseudovirus CD4 + CCR5 + HIV entry cell assay Adapted from Petropoulos CJ et al. Antimicrob Agents Chemother 2000;44:920-8.
R5 Infection R5 and X4 Variants:HIV Disease Progression Absolute Viral Load R5 X4 Limit of Detection Weeks Years Time After HIV Transmission Kuhmann SE, et al. J Viral Entry. 2005;1:4-16. Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126.
R5 Infection R5 Infection R5 and X4 Variants:HIV Disease Progression Absolute Viral Load R5 X4 Limit of Detection X4 Weeks Years Time After HIV Transmission Kuhmann SE, et al. J Viral Entry. 2005;1:4-16. Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126.
R5 Infection R5 Infection R5 and X4 Variants:HIV Disease Progression R5 + X4 Infection Absolute Viral Load R5 X4 X4 Limit of Detection Weeks Years Time After HIV Transmission Kuhmann SE, et al. J Viral Entry. 2005;1:4-16. Moore JP, et al. AIDS Res Hum Retroviruses. 2004;20:111-126.
R5 and X4 Viruses TargetDifferent Subsets of CD4+ T-Cells R5 Infection (common, early) Naïve T-Cells Relative CD4 Cell Counts Memory T-Cells Time (y) R5 viruses target memory T-cells (eg, GALT) Naïve T-cells become targets once activated to the memory phenotype Douek DC, et al. Ann Rev Immunol. 2003;21:265-304. Kuhmann SE, et al. J Viral Entry. 2005;1:4-16.
X4 Infection (very rare) Memory T-Cells Relative CD4 Cell Counts Naïve T-Cells Time (y) X4 viruses target naive T-cells (eg, thymus) CXCR4 expression on some memory cells makes them targets R5 and X4 Viruses TargetDifferent Subsets of CD4+ T-Cells R5 Infection (common, early) Naïve T-Cells Relative CD4 Cell Counts Memory T-Cells Time (y) R5 viruses target memory T-cells (eg, GALT) Naïve T-cells become targets once activated to the memory phenotype Douek DC, et al. Ann Rev Immunol. 2003;21:265-304. Kuhmann SE, et al. J Viral Entry. 2005;1:4-16.
Will a CCR5 Antagonist Drive the Emergence of X4 Viruses In Vivo? Scenario 1 CCR5 Antagonist R5 Absolute Viral Load X4 Threshold of Detection X4 Time (days) R5 viruses remain suppressed X4 viruses do not expand
Scenario 2 CCR5 Antagonist R5 X4 Viral Load X4 Threshold of Detection Time (days) R5 viruses remain suppressed Sustained, possible reciprocal expansion of X4 virus pool Will a CCR5 Antagonist Drive the Emergence of X4 Viruses In Vivo? Scenario 1 CCR5 Antagonist R5 Absolute Viral Load X4 Threshold of Detection X4 Time (days) R5 viruses remain suppressed X4 viruses do not expand
Scenario 3:Partial Expansion of the X4 Virus Pool Scenario 3 CCR5 Antagonist R5 X4 Absolute Viral Load X4 Threshold of Detection Time (days) R5 viruses remain suppressed Sustained, partial expansion of X4 virus pool
Prevalence ofHIV Co-Receptor Usage 1Fätkenheuer G, et al. Nat Med. 2005;11:1170-1172. 2Brumme ZL, et al. J Infect Dis. 2005;192:466-474. 3Moyle GJ, et al. J Infect Dis. 2005;191:866-872. 4Demarest J, et al. 44th ICAAC. Washington, DC, 2004. Abstract H-1136. 5Whitcomb JM, et al. 10th CROI. Boston, 2003. Abstract 557.
Δ32 CCR5 WT CCR5 < 1.5% < 20% ~ 80% Delayed progression Normal progression (Essentially) no progression 100 80 Genotype +/+ Genotype +/∆32 60 % AIDS free 40 n = 39 20 n = 110 0 0 2 4 6 8 10 12 14 16 18 20 Years since seroconversion Δ32 inhibition of coreceptor-mediated entry Lui R, et al.Cell 1996; 86:367–377.Samson M, et al. Nature 1996; 382:722–725.Dean M,et al. Science 1996; 273:1856–1862. Huang Y, et al.Nature Med 1996; 2:1240–1243.Michael NL, et al. Nature Med 1997; 3:1160–1162.Eugen-Olsen J,et al.AIDS 1997; 11:305–310.
Drug development Designer Drugs SAR HIV inhibition High-throughputin vitro testing Normalfunction CCR5 CXCR4 crystallography
Unknown effects of entry inhibitors Normal Function natural ligand allosteric inhibition by drug Internalisationof receptor ? Normal function ? Internalisation of receptor Viral mutations overcome
some Co-receptor antagonists have fallen by the wayside SCH-C QT AMD-3100 cardiac abnormalities but stem cell mobilization ALX 404 C no oral formulation TAK 779 toxicity at injection sites Aplaviroc hepatic side effects
Using CCR 5 antagonists Tropism shift
Impact of Current Antiretroviral Agents on R5 and X4 Virus Dynamics • In 3 cohorts, patients on HAART who were X4 or X4/R5 tropic showed a:1-4 • Preferential suppression of X4 • Shift from X4 to R5 • Loss of X4 from T-cell reservoirs in some cases • Treatment experience associated with greater risk of X4 in some cohorts5 • Acquisition of X4 virus in 8 persons homozygous for D326 • Rapid initial CD4 decline • Established wide variation in viral load “set point” • Rapid progression not invariable • Suggested behavior of X4 virus less pathogenic than in late stage • Is X4 cause or effect of progression? 1Skrabel K, et al. AIDS. 2003;107:431-438. 2Philpott S, et al. J Clin Invest. 2001;107:451-458. 3Equils O, et al. J Infect Dis. 2000;182:751-757. 4Van Rij RP, et al. J Virol. 2000;76:3054-3058. 5Demarest J, et al. 44th ICAAC. Washington, DC, 2004. Abstract H-1136. 6Sheppard HW, et al. AIDS. 2002;29:307-313.
CCR5 Antagonists:Potential Advantages • Inhibit entry of HIV-1 into host cells • Activity against viral strains resistant to current agents • Human protein target versus viral gene target • Extracellular mechanism of action
Challenges in CCR5 Antagonist Use • Utility may be related to disease stage, rather than treatment experience • Higher prevalence of X4 virus in patients with advanced disease • Trends toward later initiation of therapy may limit utility of CCR5 antagonists • Clinical trials underway to address: • Long-term safety of CCR5 inhibition • Frequency/risk/implications of X4 emergence/unmasking • Risk/benefit in patients with mixed infection • Possible need for laboratory monitoring of viral tropism?
Possible scenarios • Noninferiority proven • New class Unknown risks • Laboratory issues • ‘Superiority’ proven • Salvage – as part of last viable regimen • NRTI sparing • Substitution studies
Diflucan Partnership Program • Donation of Diflucan (fluconazole) and training of health care providers • 22 countries (915+facilities) in Africa, Asia and Caribbean participating • 67,000 patients treated for HIV-related fungal opportunistic infections • More than 18,000 health care professionals trained The Diflucan Partnership is “the first of, we hope, many other successful public/private partnerships initiated by parties who have demonstrated that they care enough to act.” — Dr. Manto Tshabalala-Msimang, Minister of Health, South Africa
International Trachoma Initiative • Public-private partnership focused on eliminating blinding trachoma • The world’s leading cause of preventable blindness • ITI now in place in 9 countries in Africa and Asia • 90% reduction in prevalence in Morocco • 50% in Tanzania • 75% in Vietnam • Donated $225 million worth of Zithromax • 10 million antibiotic treatments to date
Infectious Diseases Institute • $11 million commitment to fund regional Center of Excellence for HIV/AIDS treatment and training at Makerere University in Kampala • Extensive, one-month HIV training program for 150 physicians each year in Uganda and the region • Care and treatment for more than 50,000 patients annually • Construction of facility completed March 2004