Download
1 / 26
260 likes | 386 Views
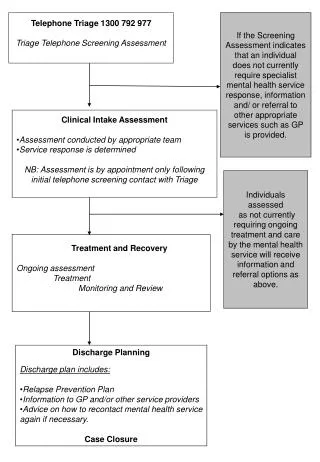
Occupational Exposure Hotline An extension of telephone triage. Allison Leonard BN RN Charlene Slaney RN. FONEMED’s Locations. Newfoundland, Canada. Remote Nurses. FONEMED. Founded in 1996

E N D
Occupational Exposure HotlineAn extension of telephone triage Allison Leonard BN RN Charlene Slaney RN
FONEMED’s Locations Newfoundland, Canada Remote Nurses
FONEMED • Founded in 1996 • Provides nurse triage for 150 clients and 2,100 physicians, covering more than 8,000,000 people throughout the US, Canada and the Caribbean. • Fully URAC accredited since 2000 • Call centers opened in: Canada; Puerto Rico; Philippines; Greece; Ecuador; Dominican Republic and Bangladesh • Occupational Exposure Hotline services since 2006
Introduction • Health care providers, first responders and law enforcement professionals face serious safety issues when they find themselves exposed to health-threatening incidents on the job. • Rapid, reliable and documented guidance by specially-trained medical personnel is essential to the safety of the exposed person and, frequently, others with whom he or she is in contact.
Exposure Hotline Clients Employees of: • Hospitals/Doctors Offices • Dentist Offices • Municipal Employees/ First Responders (Fire, Police, EMS) • Correctional Facilities • Rehab Centers • Dialysis Centers
Interesting Facts • The average risk of HIV infection after a needlestick or cut exposure to HlV-infected blood is 0.3% • The risk after exposure of the eye, nose, or mouth to HIV-infected blood is estimated to be, on average, 0.1% • The risk after exposure of non-intact skin to HlV-infected blood is estimated to be less than 0.1% • Healthcare personnel who have received Hepatitis B vaccine and developed immunity to the virus are at virtually no risk for infection. For a susceptible person, the risk from a single needlestick or cut exposure to Hepatitis B infected blood ranges from 6-30% • The average risk for infection after a needlestick or cut to Hepatitis C infected blood is approximately 1.8%
Interesting Facts (cont) • Scientists and medical authorities agree that HIV does not survive well in the environment, making the possibility of environmental transmission remote. In fact, drying of HIV-infected human blood or other body fluids reduces the theoretical risk of environmental transmission to essentially zero • The Hepatitis B Virus (HBV) can survive outside the body at least 7 days and still be capable of causing infection • The Hepatitis C Virus (HCV) can survive outside the body at room temperature, on environmental surfaces, for at least 16 hours but no longer than 4 days
What is an Occupational Exposure? Theexposure to potentially harmfulchemical, physical, or biological agents that occurs as a result of one's occupation. Exposure Hotline Classifications: 1. Blood and Body Fluid Exposure 2. Communicable Disease Exposure 3. Unusual Exposure
Hotline Classifications of Exposures 1. BBFE (Blood or Body Fluid Exposure) a) Infectious - Contact with BLOOD or Other Potentially Infectious Material (OPIM) • Pericardial fluid • Synovial fluid • Pleural fluid • Tissue • Vaginal Secretions • Semen b) Non-Infectious – Contact with Non-Potentially Infectious Material (non-OPIM) • Emesis • Sweat • Saliva • Nasal secretions and Sputum • Urine and Stool
BBFE: Definition of “Contact” • Contact Methods or Ports of Entry: • Percutaneous Injury • Mucus membrane • Non-intact skin • Human bite
BBFE: Why The Concern? Blood & OPIM’s may contain pathogens that are deadly: • HIV/AIDS • Hepatitis B • Hepatitis C Non–OPIMs are not considered significant exposures with the risk of disease transmission unless fluids contain visible blood or a high likelihood of blood being present
Hotline Classifications of Exposures (cont) 2. Communicable Disease Exposure Transmitted by an infected person through a specific agent or its toxic products to a susceptible host. • Meningitis • TB • MRSA • Chicken Pox • Shingles • Influenza A • H1N1 • Scabies • Hepatitis A
Hotline Classifications of Exposures (cont) 3. Unusual Exposures Hotline Nurse will contact Licensed Health Risk Manager (LHRM); an on-call Occupational Medicine Physician will be consulted as needed. Client will be called by LHRM or Physician with recommendations for treatment and/or follow up. • SARS • Ebola • Mold • Chemicals • Fumes • Chemotherapeutic agents
BBFE Recommendations • Because individual exposure incidents are so unique, each exposure situation must be evaluated on an individual basis. • The exposure hotline nurse evaluates the blood and body fluid exposure to determine the need for surveillance, counseling and Post Exposure Prophylactic (PEP) medications based on CDC guidelines. • These Recommendations depend on whether the body fluid is considered infectious and if there is a port of entry.
Surveillance & Counseling Surveillance Complete initial baseline blood work for EE now (or ASAP), followed by repeat blood work in 6 weeks, 12 weeks, 6 months. • EE blood work to include: • Screen for HIV Antibody Titre • Screen for Hep B virus • Screen for Hep C antibody Titre • Additional testing deemed necessary for further treatment (hepatic function testing, pregnancy testing, etc) • Source Testing to include: • RAPID HIV testing • Additional source testing for HIV, Hepatitis B and Hepatitis C Counseling (During Surveillance Period): • Practice safer sex using latex condom – use plastic if allergic to latex • Do not donate blood, blood products, organ, tissue (or semen for male) • Women of child bearing age: Avoid pregnancy and discontinue breastfeeding
HIV PEP Medications • Post exposure prophylaxis (PEP) is recommended for certain occupational exposures that pose a risk of HIV transmission. • Options for PEP should be discussed with Health Care Provider; start PEP if source is high risk; discontinue medications when source confirmed negative. • 4-week course of a combination of either two antiretroviral drugs for most HIV exposures, or three antiretroviral drugs for exposures that may pose a greater risk for transmitting HIV • Treatment should be started as soon as possible, preferably within hours as opposed to days, after the exposure. • All of the antiviral drugs for treatment of HIV have been associated with side effects. The most common side effects include upset stomach (nausea, vomiting, diarrhea), tiredness, or headache. The few serious side effects that have been reported in healthcare personnel using combinations of antiviral drugs after exposure have included kidney stones, hepatitis, and suppressed blood cell production
Hepatitis B & C Exposure Recommendations • HBIG and/or Hepatitis B vaccine may be recommended depending on the source’s infection status, employee’s vaccination status and, if vaccinated, the response to the vaccine • If not vaccinated, Hepatitis B vaccination is recommended for any exposure regardless of the source person’s HBV status. • Post exposure treatment should begin as soon as possible after exposure, preferably within 24 hours, and no later than 7 days. • After receiving Hepatitis B vaccine, testing should be completed 1-2 months after vaccine series to determine response to the vaccine and if employee is protected against HBV infection. • There is no vaccine against Hepatitis C and no treatment after an exposure that will prevent infection.
Communicable Disease Exposure Recommendations • Treatment and follow up recommendations depend on particular disease/illness of exposure • Generally no testing needed (except TB), unless symptoms develop • Preventative medications or vaccines may be ordered with or without symptoms
Unusual Exposure Recommendations • Recommendations, treatment and follow up instructions to be determined by on call Licensed Health Risk Manager or Occupational Medicine Physician • Employees may be directed to seek treatment immediately with Health Care Provider • If applicable, Instructions/Teaching on “what to look for” to be verbalized to employee.
Exposure Hotline Goals • Primary goal is to assure that callers in each of the three exposure categories receive immediate guidance from qualified medical personnel using best practice medical protocols to direct them to an appropriate response to their specific safety concern. • Secondary goals of the Occupational Exposure Hotline include identification of broader health risks to the public, documentation of all incidents, and ongoing collaboration with public health authorities to improve outcomes.
Patient & Risk Assessment • Registered Nurses are on standby 24/7 to take calls from exposed personnel and walk them through the process of reporting and managing their exposure. • Using custom-designed software and over 1200 CDC protocols, nurses are able to assess the severity of an exposure and the proper steps to take following the exposure • Reports are sent to treating Health Care Providers, outlining CDC recommendations for treatment
Data Elements Gathered from Callers • Employee information: Legal name, DOB, SSN, home address and contact information, etc … • Employer information: Employer name, employer address, supervisor information, date of hire, etc… • Incident details: Description of the incident, when it occurred, what first aid measures were taken after • Immunization history • Source information - contact information, medical history, HIV, Hep B & C status • Risk factors
Care Management & Documentation • After the exposure, many times the exposed person has questions about how to manage their reactions to the substance they were exposed to. Nurses are trained to answer those questions. • Doctors and Registered Nurses work together to document the caller's exposure.
Information Provided to Callers / HCP • CDC recommendations for treatment and follow-up • Information from the Employer on authorized treating health care providers (we can direct the employee on where to go for treatment and forward all recommendations to that treating HCP)
Occupational Exposure Prevention • Following appropriate vaccination schedules - Hepatitis B virus is largely preventable through vaccination. • Preventing occupational exposures to blood, body fluids and communicable diseases can prevent occupational infections • Using appropriate barriers such as gown, gloves, mask and eye protection as appropriate • Safe handling of needles and other sharp instruments • Safe disposal of body fluids • Using devices with safety features • Hand washing
THANK YOU! Allison Leonard BN RN aleonard@fonemed.com Charlene Slaney RN cslaney@fonemed.com