Download
1 / 1
10 likes | 101 Views
Creatinine Clearance in Cystic Fibrosis patients: aMDRD, Cockcroft-Gault and measured Creatinine Clearance. Bronsveld I, Conemans L.H., Teding van Berkhout F., Boerhof E., Zanen P., van de Graaf E.A., Lammers J-W.J. University Medical Center Utrecht, The Netherlands. Introduction

E N D
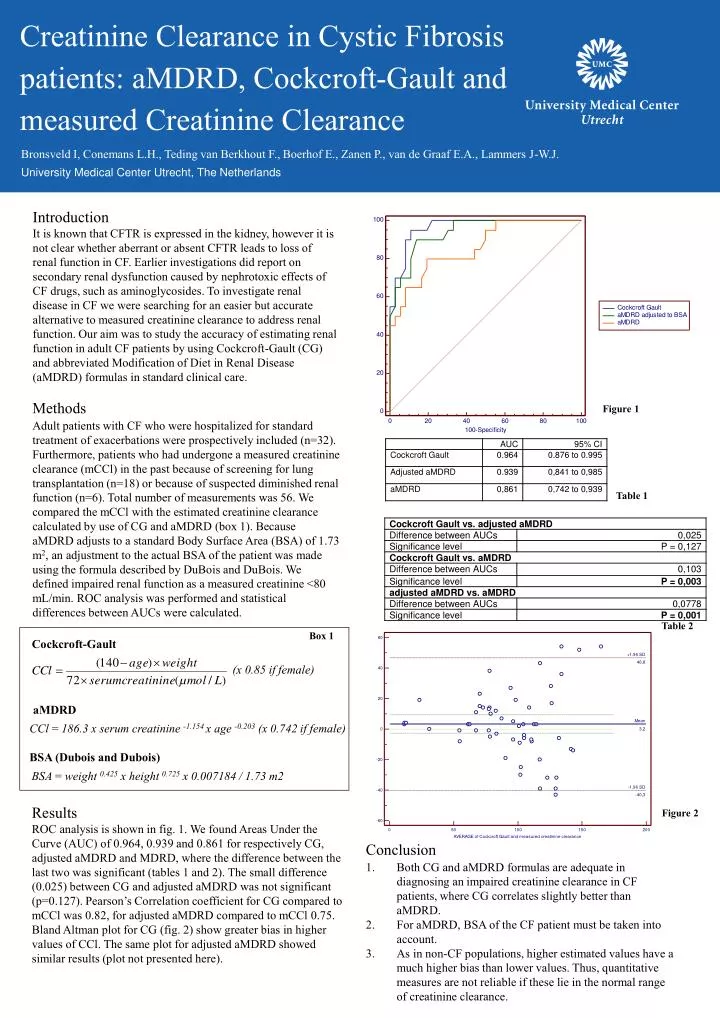
Creatinine Clearance in Cystic Fibrosis patients: aMDRD, Cockcroft-Gault and measured Creatinine Clearance Bronsveld I, Conemans L.H., Teding van Berkhout F., Boerhof E., Zanen P., van de Graaf E.A., Lammers J-W.J. University Medical Center Utrecht, The Netherlands Introduction It is known that CFTR is expressed in the kidney, however it is not clear whether aberrant or absent CFTR leads to loss of renal function in CF. Earlier investigations did report on secondary renal dysfunction caused by nephrotoxic effects of CF drugs, such as aminoglycosides. To investigate renal disease in CF we were searching for an easier but accurate alternative to measured creatinine clearance to address renal function. Our aim was to study the accuracy of estimating renal function in adult CF patients by using Cockcroft-Gault (CG) and abbreviated Modification of Diet in Renal Disease (aMDRD) formulas in standard clinical care. Methods Adult patients with CF who were hospitalized for standard treatment of exacerbations were prospectively included (n=32). Furthermore, patients who had undergone a measured creatinine clearance (mCCl) in the past because of screening for lung transplantation (n=18) or because of suspected diminished renal function (n=6). Total number of measurements was 56. We compared the mCCl with the estimated creatinine clearance calculated by use of CG and aMDRD (box 1). Because aMDRD adjusts to a standard Body Surface Area (BSA) of 1.73 m2, an adjustment to the actual BSA of the patient was made using the formula described by DuBois and DuBois. We defined impaired renal function as a measured creatinine <80 mL/min. ROC analysis was performed and statistical differences between AUCs were calculated. Figure 1 Table 1 Table 2 Box 1 Cockcroft-Gault (x 0.85 if female) aMDRD CCl = 186.3 x serum creatinine -1.154 x age -0.203 (x 0.742 if female) BSA (Dubois and Dubois) BSA = weight 0.425 x height 0.725 x 0.007184 / 1.73 m2 Results ROC analysis is shown in fig. 1. We found Areas Under the Curve (AUC) of 0.964, 0.939 and 0.861 for respectively CG, adjusted aMDRD and MDRD, where the difference between the last two was significant (tables 1 and 2). The small difference (0.025) between CG and adjusted aMDRD was not significant (p=0.127). Pearson’s Correlation coefficient for CG compared to mCCl was 0.82, for adjusted aMDRD compared to mCCl 0.75. Bland Altman plot for CG (fig. 2) show greater bias in higher values of CCl. The same plot for adjusted aMDRD showed similar results (plot not presented here). Figure 2 • Conclusion • Both CG and aMDRD formulas are adequate in diagnosing an impaired creatinine clearance in CF patients, where CG correlates slightly better than aMDRD. • For aMDRD, BSA of the CF patient must be taken into account. • 3. As in non-CF populations, higher estimated values have a much higher bias than lower values. Thus, quantitative measures are not reliable if these lie in the normal range of creatinine clearance.