Download
1 / 1
10 likes | 167 Views
Paul A. Pham 1830 E. Monument Street Room 444 Baltimore, MD 21287 Phone: 410-502-4342 Email: vpham@jhmi.edu. Poster # A-381 ICAAC 2006 San Francisco, CA. Amprenavir (APV) and Lopinavir (LPV) Pharmacokinetics (PK) in

E N D
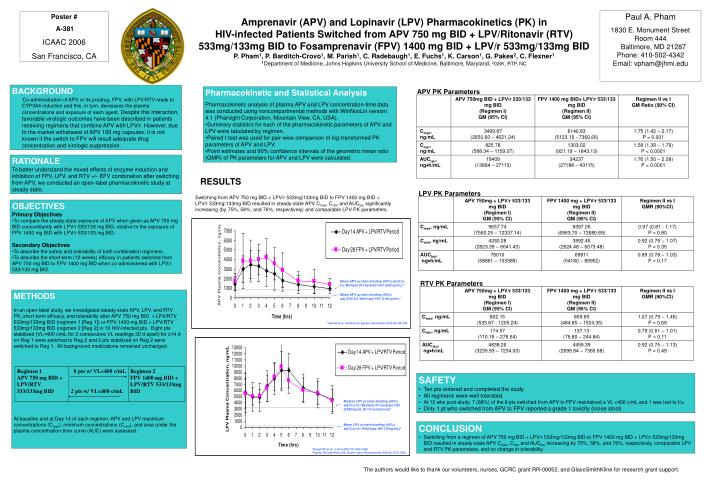
Paul A. Pham 1830 E. Monument Street Room 444 Baltimore, MD 21287Phone: 410-502-4342Email: vpham@jhmi.edu Poster # A-381 ICAAC 2006 San Francisco, CA Amprenavir (APV) and Lopinavir (LPV) Pharmacokinetics (PK) in HIV-infected Patients Switched from APV 750 mg BID + LPV/Ritonavir (RTV) 533mg/133mg BID to Fosamprenavir (FPV) 1400 mg BID + LPV/r 533mg/133mg BID P. Pham1, P. Barditch-Crovo1, M. Parish1, C. Radebaugh1, E. Fuchs1, K. Carson1, G. Pakes2, C. Flexner1 1Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland, 2GSK, RTP, NC BACKGROUND Co-administration of APV or its prodrug, FPV, with LPV/RTV leads to CYP3A4 induction and this, in turn, decreases the plasma concentrations and exposure of each agent. Despite this interaction, favorable virologic outcomes have been described in patients receiving regimens that combine APV with LPV/r. However, due to the market withdrawal of APV 150 mg capsules, it is not known if the switch to FPV will result adequate drug concentration and virologic suppression. • Pharmacokinetic and Statistical Analysis • Pharmacokinetic analysis of plasma APV and LPV concentration-time data was conducted using noncompartmental methods with WinNonLin version 4.1 (Pharsight Corporation, Mountain View, CA, USA). • Summary statistics for each of the pharmacokinetic parameters of APV and LPV were tabulated by regimen. • Paired t-test was used for pair-wise comparison of log-transformed PK parameters of APV and LPV. • Point estimates and 90% confidence intervals of the geometric mean ratio (GMR) of PK parameters for APV and LPV were calculated. APV PK Parameters RATIONALE To better understand the mixed effects of enzyme induction and inhibition of FPV, LPV, and RTV +/- EFV combination after switching from APV, we conducted an open-label pharmacokinetic study at steady state. RESULTS LPV PK Parameters Switching from APV 750 mg BID + LPV/r 533mg/133mg BID to FPV 1400 mg BID + LPV/r 533mg/133mg BID resulted in steady-state APV Cmax, Cmin and AUCtau significantly increasing (by 75%, 58%, and 76%, respectively) and comparable LPV PK parameters. • OBJECTIVES • Primary Objectives • To compare the steady-state exposure of APV when given as APV 750 mg BID concomitantly with LPV/r 533/133 mg BID, relative to the exposure of FPV 1400 mg BID with LPV/r 533/133 mg BID. • Secondary Objectives • To describe the safety and tolerability of both combination regimens. • To describe the short-term (12 weeks) efficacy in patients switched from APV 750 mg BID to FPV 1400 mg BID when co-administered with LPV/r 533/133 mg BID. Mean APV protein-binding (90%) adj IC50 forMultiple PI-resistant HIV (900ng/mL)* RTV PK Parameters ← ----------------------------------------------------------- METHODS In an open-label study, we investigated steady-state APV, LPV, and RTV PK, short-term efficacy, and tolerability after APV 750 mg BID + LPV/RTV 533mg/133mg BID (regimen 1 [Reg 1]) or FPV 1400 mg BID + LPV/RTV 533mg/133mg BID (regimen 2 [Reg 2] in 10 HIV-infected pts. Eight pts stabilized (VL<400 c/mL for 2 consecutive VL readings 30 d apart) for ≥14 d on Reg 1 were switched to Reg 2 and 2 pts stabilized on Reg 2 were switched to Reg 1. All background medications remained unchanged. At baseline and at Day 14 of each regimen, APV and LPV maximum concentrations (Cmax), minimum concentrations (Cmin), and area under the plasma concentration-time curve (AUC) were assessed. ← ----------------------------------------------------------- Mean APV protein-binding (90%) adj IC50 for Wild-type HIV (146ng/mL) * *Sale M et al: Antimicrob Agents Chemother 2002;46:746-754. • SAFETY • Ten pts entered and completed the study • All regimens were well tolerated. • At 12 wks post-study, 7 (88%) of the 8 pts switched from APV to FPV maintained a VL <400 c/mL and 1 was lost to f/u. • Only 1 pt who switched from APV to FPV reported a grade 1 toxicity (loose stool) Median LPV protein-binding (90%) adj IC50 for Multiple PI-resistant HIV (3080ng/mL [8-10 mutations])* ← ------------------------------------------------------ ------------------------------------------------------- ← Mean LPV protein-binding (90%) adj IC50 for Wild-type HIV (70ng/mL)† • CONCLUSION • Switching from a regimen of APV 750 mg BID + LPV/r 533mg/133mg BID to FPV 1400 mg BID + LPV/r 533mg/133mg BID resulted in steady-state APV Cmax, Cmin and AUCtau increasing by 75%, 58%, and 76%, respectively, comparable LPV and RTV PK parameters, and no change in tolerability. *Kempf DF et al: J Virol 2001;75:7462-7469. †Kaplan SS and Hicks CB: Expert Opin Pharmacother 2005;6:1573-1585. The authors would like to thank our volunteers, nurses, GCRC grant RR-00052, and GlaxoSmithKline for research grant support.