Download
1 / 25
260 likes | 426 Views
CONGENITAL HEART DEFECTS D. HANA OMER. The major development of the fetal heart occurs between the fourth and seventh weeks of gestation, and most congenital heart defects arise during this time .

E N D
CONGENITAL HEART DEFECTS D. HANA OMER
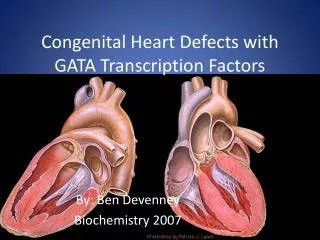
The major development of the fetal heart occurs between the fourth and seventh weeks of gestation, and most congenital heart defects arise during this time. • resulting from an interaction between a genetic predisposition toward development of a heart defect and environmental influences. • Approximately 13% of children with congenital heart disease have an associated chromosomal abnormality. • maternal conditions and teratogenic influences, including maternal diabetes, congenital rubella, maternal alcohol ingestion, and treatment with anticonvulsant drugs.
Acyanotic and Cyanotic Disorders • It is devided into cyanotic and acyanotic disorders . • Left-to-right shunts commonly are categorized as acyanoticdisorders and right-to left shunts are cyanotic disorders. • Shunting of blood refers to the diverting of blood flow from one system to the other from the arterial to the venous system (i.e., left-to-right shunt) or from the venous to the arterial system (i.e., right-to-left shunt).
CYANOTIC HEART DISEASE • Tetralogy of fallots. • Transposition of great arteries (TGA). • Tricuspid atresia. • Truncusarteriosus. • Eisenmenger’s syndrome.
Acyanotic Disorders • With left to right shunt :- • Atrialseptal defect (ASD). • Ventricular septal defect (VSD). • Patent ductusarteriosis. • With no shunt :- • Coarctation of aorta. • Congenital aortic stenosis. • Pulmonary stenosis, tricuspid stenosis. • Ebstein’sanamoly. • Dextrocardia.
Almost all mitral stenosis is due to rheumatic heart disease . • Rheumatic mitral stenosis is much more common in women (about 1/3 case) . • Rare causes of mitral stenosis may be congenital, or because calcification and fibrosis of the valve in elderly .
PATHOPHYSIOLOGY • The commisures of mitral valve become adherent and the chordaetendinae are short and deformed . • The normal mitral valve orifice is about 4-6 cm² in diastole, it is reduced to about 1 cm² in severe mitral stenosis. • left atrial , pulmonary venous, pulmonary capillary pressure. • Also result in atrial fibrillation pulmonary edema pulmonary hypertension . • All cases may develop pulmonary hypertension and right ventricular hypertrophy .
All patients with mitral stenosis are at risk of left atrial thrombosis and systemic thromboembolism . • Mitral stenosis is frequently associated with mitral regurgitation or disease of the aortic or tricuspid valve .
SYMPTOMS • DYSPNEA . • COUGH . • PALPITATION . • FEATURES OF CHRONIC RIGHT HEART FAILURE .
ON EXAMINATION • INSPECTION : left parasternal pulsation due to right ventricular hypertrophy . • PALPATION : • Apex beat not displaced . • Tapping apex beat . • Left parasternal heave . • Palpable P₂ . • AUSCULTATION : HEART SOUNDS : • Loud first heart sound . • Loud P₂. • Opening snap .
MURMURS : • Mid-diastolic rumbling murmur . • Pre-systolic accentuation of murmur .
COMPLICATION • ATRIAL FIBRILLATION . • SYSTEMIC EMBOLIZATION . • PULMONARY HYPERTENSION . • PULMONARY INFARCTION . • INFECTIVE ENDOCARDITIS . • TRICUSPID REGURGITATION . • RIGHT VENTRICULAR FAILURE .
X-RAY CHEST : • Double shadow behind right heart :enlarged left atrium . • Kerley’s B lines : which are small 1-2 cm horizontal lines present in the costohrenic angle appearing due to raised pulmonary venous pressure . • ECG . • ECO .
MEDICAL TREATMENT • MILD DYSPNEA : salt restriction, low doses of diuretics . • SINUS RHYTHM : beta blockers . • ATRIAL FIBRILLATION : beta blockers, calaium channel blocker • Prphylactic antibiotics to prevent infective endocarditis .
SURGICAL TREATMENT • PERCUTANEOUS TRANSLUMINAL MITRAL COMMISSUROTOMY (PTMC) : • INDICATIONS: • Uncontrolled pulmonary edema . • Symptoms of pulmonary congestion persist despite therapy . • Recurrent systemic emboli despite anticoagulation .