Download
1 / 38
450 likes | 885 Views
INTRAMEDULLARY SPINAL CORD TUMORS. K. Liaropoulos, P. Spyropoulou, N. Papadakis 3rd Neurosurgery clinic, Athens Euroclinic. EPIDEMIOLOGY. 2-4% of tumors in the CNS in adults and children Exception: the first year of life (Around 12%). ORIGIN. Most tumors are of glial origin

E N D
INTRAMEDULLARY SPINAL CORD TUMORS K. Liaropoulos, P. Spyropoulou, N. Papadakis 3rd Neurosurgery clinic, Athens Euroclinic
EPIDEMIOLOGY • 2-4% of tumors in the CNS in adults and children • Exception: the first year of life (Around 12%)
ORIGIN Most tumors are of glial origin • Ependymoma (52%) • Astrocytoma (46%)
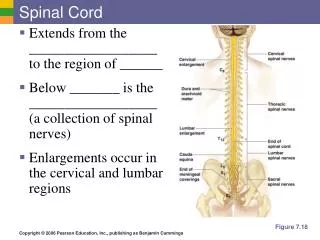
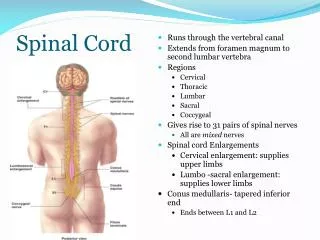
LOCALIZATION IN THE SPINAL CORD • cervicobulbar 11% • cervical 24% • cervicothoracic 25% • thoracic 22% • thoracolumbar 13% • total 5%
SYMPTOMS a) Pain (back or radicular) b) Paresthesia c) Scoliosis (in children)
CLINICAL PROFILE • Torticollis • Motor deficit • Sphincter disorders
Neurological examination • Hypoaesthesia • Motor deficit • Pyramidal syndrome
HISTOLOGICAL EXAMINATION A) EPENDYMOMA According to the World Health Organization (WHO) • of 2nd grade (90%) • rarely of 3rd grade B) ASTROCYTOMA • most of 2nd grade • rarely of 3rd grade • glioblastomas very rare
NEURORADIOLOGY A) Radiography • Very limited contribution B) Myelography • Indirect diagnosis due to swelling of the spinal cord • Does not indicate the characteristics of the lesion • Invasive examination C) Computed tomography • Limited contribution
Advantages of MRI In most cases it contributes to: A) Localization B) Size C) Solid - cystic components D) Composition some times (Lipoma, cavernous hemangioma)
ATTENTION! MRI can not distinguish between astrocytoma and ependymoma with any degree of accuracy.
TREATMENT • The main treatment is surgery
SURGICAL TECHNIQUE • Position: prone • laminectomy / laminotomy • Exposure of dura mater • Exposure of arachnoid mater (With microscissors)
Overview of the spinal cord (swelling - change in the color) • Localization of posterior median fissure (sometimes difficult)
Overview of the spinal cord • (swelling - change in the color) • Localization of posterior median • fissure (sometimes difficult)
Exposure of spinal cord • Biopsy • Ultrasound-guided resection • Detailed haemostasis • Suture
COMPLICATIONS A) Sensory: Change little after the third month B) Motor: Typically improve by 1 ½ years
IMPORTANT In the best case scenario the long-term neurological condition will be the same as the condition that first drove the patient to the doctor
RADIOTHERAPY • We mention it last in order to emphasize that we do not believe there is any reason for this method, unless for treatment of malignant tumors, especially in children. • Even in these cases its value and safety have yet to be proved.
SUMMARY AND CONCLUSIONS • There is no pathognomonic profile of intramedullary tumors. However, pain in the back or neck or radicular pain or diffuse dysesthesia, are always the first signs of an intramedullary tumor
The MRI is the preferred screening test and should include full sections and the injection of contrast medium. Only the following cases present a characteristic picture: Hemangioblastoma, dermoid cysts, epidermoid cysts and lipomas
2/3 of intramedullary tumors are of glial origin. Sometimes the histological verification is difficult and requires additional staining and immunohistochemical techniques
The operation of intramedullary tumors is guided by the anatomy and relies on the access through the posterior median fissure. The main risk is lesion (Temporary or permanent) of the posterior column in 70% of cases
The resection of intramedullary tumors is currently performed with CUSA. Laser is not indicated because it blackens the surgical field and characteristics of the intramedullary tumor are lost
The main goal of the surgery of intramedullary tumors is total resection. This is possible only when there is a separating region between the intramedullary tumor and the spinal cord. In absence thereof, total resection is impossible and such attempt is dangerous and unnecessary.
If the tumor is astrocytoma, the prognosis is not necessarily hopeless. Approximately 50% are totally resectable
When the MRI indicates the presence of an intramedullary tumor, surgery is necessary since even completely benign tumors have been resected in patients where the MRI is referred to as invasive type of diagnostics
Radiotherapy is contraindicated in dealing with intramedullary tumors
The low mortality, morbidity and recurrence of intramedullary tumors constitute surgery the only effective treatment for intramedullary tumors.