Download
1 / 18
571 likes | 3.53k Views
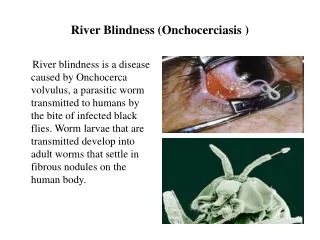
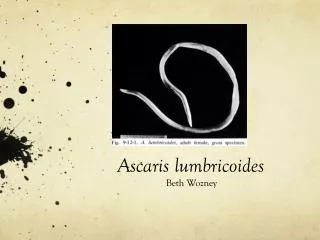
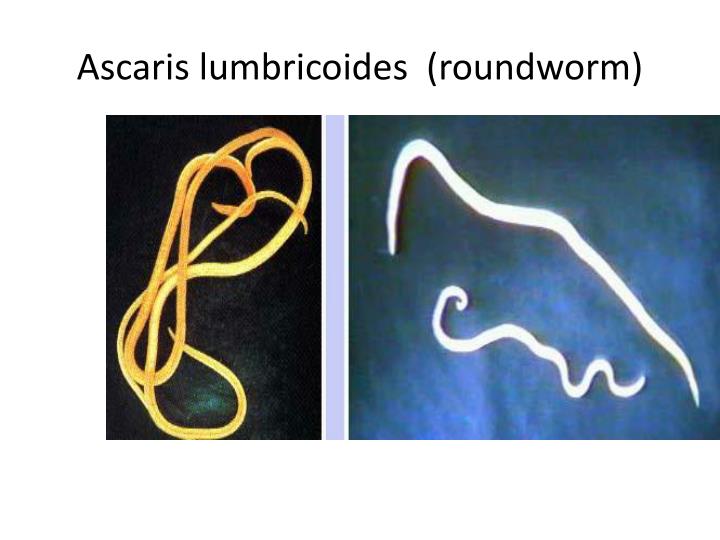
Ascaris lumbricoides (roundworm). Introduction. Most common helminthic human infection Largest nematode to infect the human intestine An estimated 1 billion people are infected (1 out of 4 people in the world). Geography. Worldwide

E N D
Introduction • Most common helminthic human infection • Largest nematode to infect the human intestine • An estimated 1 billion people are infected (1 out of 4 people in the world)
Geography • Worldwide • High prevalence in underdeveloped countries that have poor sanitation (parts of Asia, South America and Africa) • Occurs during rainy months, tropical and subtropical countries
Factors favoring the spread of the transmission: 1. Simple life cycle. 2. Enormous egg production ( 240,000 eggs/ day/ female ). 3. These eggs are highly resistant to ordinary disinfectants( due to the ascroside). The eggs may remain viable for several years. 5. Disposal of feces is unsuitable.
Host • Definitive host : Humans or pigs • Intermediate Host : -none-
Modes of transmission • Occurs mainly via ingestion of water or food (raw vegetables or fruit in particular) contaminated with A. lumbricoides eggs. • Occasionally inhalation of contaminated dust • Children playing in contaminated soil may acquire the parasite from their hands • Enhanced by the fact that individuals can be asymptomatically infected and continues to shed eggs for years • Prior infection does not confer protective immunity
II Life Cycle • 1.Site of inhabitation: small intestine 2. Infective stage: embryonated eggs 3. Route of infection: by mouth 4. No intermediate and reservoir hosts 5. Life span of the adult: about 1 year This worm lives in the lumen of small intestine, feeding on the intestinal contents, where the fertilized female lays eggs. An adult female can produce approximately 240,000 eggs per day, which are passed in feces. When passed, the eggs are unsegmented and require outside development of about three weeks until a motile embryo is formed within the egg.
After the ingestion of embryonated eggs in contaminated food or drink or from contaminated fingers, host digestive juices acts on the egg shell and liberate the larva into the small intestine. These larvae penetrate the intestinal mucosa and enter lymphatics and mesenteric vessels. They are carried by circulation to the liver, right heart and finally to the lungs where they penetrate the capillaries into the alveoli in which they molt twice and stay for 10-14days and then they are carried, or migrate, up the bronchioles, bronchi, and trachea to the epiglottis.
When swallowed, the larvae pass down into the small intestine where they develop into adults. The adult worms live for about one year.
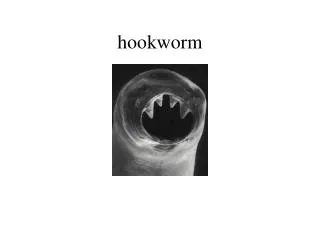
Food Habits • Feeds on semi-digested contents in the gut • Evidence show that they can bite the intestinal mucus membrane and feed on blood and tissue fluids
Symptoms Symptoms associated with larvae migration • Migration of larvae in lungs may cause hemorrhagic/ eosinophilic pneumonia, cough (Loeffler's Syndrome) • Breathing difficulties and fever • Complications caused by parasite proteins that are highly allergenic - asthmatic attacks, pulmonary infiltration and urticaria .
Symptoms Cont. Symptoms associated with adult parasite in the intestine • Usually asymptomatic • Abdominal discomfort, nausea in mild cases • Malnutrition in host especially children in severe • Sometimes fatality may occur when mass of worm blocks the intestine
Diagnosis • Stool microscopy :eggs may be seen on direct examination of feces . Eggs are round or oval, brownish,with a thick covering. • Eosinophilia: eosinophilia can be found, particularly during larval migration through the lungs • Imaging: In heavily infested individuals, particularly children, large collections of worms may be detectable on plain film of the abdomen. • Ultrasound: ultrasound exams can help to diagnose hepatobiliary or pancreatic ascariasis. Single worms, bundles of worms, or pseudotumor-like appearance, individual body segments of worms may be seen.
Treatment • Mebendazole-- (100 mg twice a day for three days) • Albendazole -400 mg • Pyrantel pamoate (single dose 11mg / kg ) • Piperazine citrate- (150 mg/kg stat followed by 65 mg/kgat 12 hr interval for 6 dose) • Severe obst. may require surgery.
Prevention • Prevention of reinfection poses a substantial problem since this parasite is abundant in soil – therefore good sanitation is needed to prevent fecal contamination of soil • Limit using human feces as fertilizer • Treatment can be done on contaminated soil although it is not highly advised • Mass treatments of children with single doses of mebendazole or albendazole – helps reduce transmission in community but can cause reinfection