Download
1 / 1
10 likes | 124 Views
Switching vs. Consistent Triptan Treatment and Headache-Related Disability: Results of the American Migraine Prevalence and Prevention (AMPP) Study

E N D
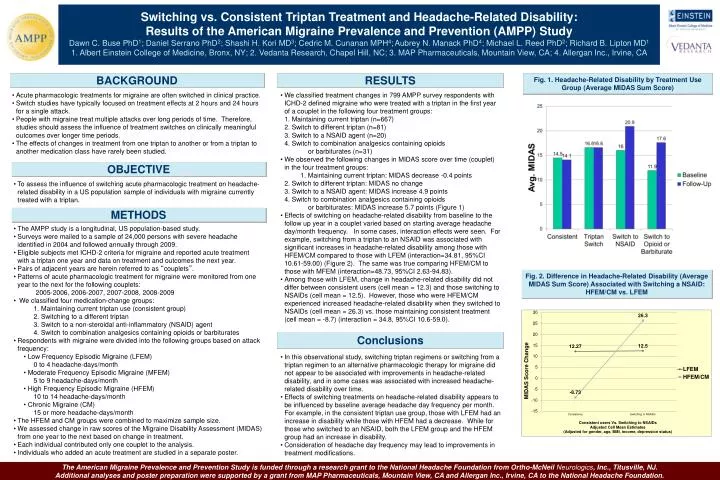
Switching vs. Consistent Triptan Treatment and Headache-Related Disability: Results of the American Migraine Prevalence and Prevention (AMPP) Study Dawn C. Buse PhD1; Daniel Serrano PhD2; Shashi H. Kori MD3; Cedric M. Cunanan MPH4;Aubrey N. Manack PhD4; Michael L. Reed PhD2; Richard B. Lipton MD1 1. Albert Einstein College of Medicine, Bronx, NY; 2. Vedanta Research, Chapel Hill, NC; 3. MAP Pharmaceuticals, Mountain View, CA; 4. Allergan Inc., Irvine, CA BACKGROUND RESULTS Fig. 1. Headache-Related Disability by Treatment Use Group (Average MIDAS Sum Score) • Acute pharmacologic treatments for migraine are often switched in clinical practice. • Switch studies have typically focused on treatment effects at 2 hours and 24 hours for a single attack. • People with migraine treat multiple attacks over long periods of time. Therefore,studies should assess the influence of treatment switches on clinically meaningful outcomes over longer time periods. • The effects of changes in treatment from one triptan to another or from a triptan to another medication class have rarely been studied. • We classified treatment changes in 799 AMPP survey respondents with ICHD-2 defined migraine who were treated with a triptan in the first year of a couplet in the following four treatment groups: 1. Maintaining current triptan (n=667) 2. Switch to different triptan (n=81) 3. Switch to a NSAID agent (n=20) 4. Switch to combination analgesics containing opioids or barbiturates (n=31) • We observed the following changes in MIDAS score over time (couplet) in the four treatment groups: 1. Maintaining current triptan: MIDAS decrease -0.4 points 2. Switch to different triptan: MIDAS no change 3. Switch to a NSAID agent: MIDAS increase 4.9 points 4. Switch to combination analgesics containing opioids or barbiturates: MIDAS increase 5.7 points (Figure 1) • Effects of switching on headache-related disability from baseline to the follow up year in a couplet varied based on starting average headache day/month frequency. In some cases, interaction effects were seen. For example, switching from a triptan to an NSAID was associated with significant increases in headache-related disability among those with HFEM/CM compared to those with LFEM (interaction=34.81, 95%CI 10.61-59.00) (Figure 2). The same was true comparing HFEM/CM to those with MFEM (interaction=48.73, 95%CI 2.63-94.83). • Among those with LFEM, change in headache-related disability did not differ between consistent users (cell mean = 12.3) and those switching to NSAIDs (cell mean = 12.5). However, those who were HFEM/CM experienced increased headache-related disability when they switched to NSAIDs (cell mean = 26.3) vs. those maintaining consistent treatment (cell mean = -8.7) (interaction = 34.8, 95%CI 10.6-59.0). OBJECTIVE • To assess the influence of switching acute pharmacologic treatment on headache-related disability in a US population sample of individuals with migraine currently treated with a triptan. METHODS • The AMPP study is a longitudinal, US population-based study. • Surveys were mailed to a sample of 24,000 persons with severe headache identified in 2004 and followed annually through 2009. • Eligible subjects met ICHD-2 criteria for migraine and reported acute treatment with a triptan one year and data on treatment and outcomes the next year. • Pairs of adjacent years are herein referred to as “couplets”. • Patterns of acute pharmacologic treatment for migraine were monitored from one year to the next for the following couplets: 2005-2006, 2006-2007, 2007-2008, 2008-2009 • We classified four medication-change groups: 1. Maintaining current triptan use (consistent group) 2. Switching to a different triptan 3. Switch to a non-steroidal anti-inflammatory (NSAID) agent 4. Switch to combination analgesics containing opioids or barbiturates • Respondents with migraine were divided into the following groups based on attack frequency: • Low Frequency Episodic Migraine (LFEM) 0 to 4 headache-days/month • Moderate Frequency Episodic Migraine (MFEM) 5 to 9 headache-days/month • High Frequency Episodic Migraine (HFEM) 10 to 14 headache-days/month • Chronic Migraine (CM) 15 or more headache-days/month • The HFEM and CM groups were combined to maximize sample size. • We assessed change in raw scores of the Migraine Disability Assessment (MIDAS) from one year to the next based on change in treatment. • Each individual contributed only one couplet to the analysis. • Individuals who added an acute treatment are studied in a separate poster. Fig. 2. Difference in Headache-Related Disability (Average MIDAS Sum Score) Associated with Switching a NSAID: HFEM/CM vs. LFEM Conclusions • In this observational study, switching triptan regimens or switching from a triptan regimen to an alternative pharmacologic therapy for migraine did not appear to be associated with improvements in headache-related disability, and in some cases was associated with increased headache-related disability over time. • Effects of switching treatments on headache-related disability appears to be influenced by baseline average headache day frequency per month. For example, in the consistent triptan use group, those with LFEM had an increase in disability while those with HFEM had a decrease. While for those who switched to an NSAID, both the LFEM group and the HFEM group had an increase in disability. • Consideration of headache day frequency may lead to improvements in treatment modifications. The American Migraine Prevalence and Prevention Study is funded through a research grant to the National Headache Foundation from Ortho-McNeil Neurologics, Inc., Titusville, NJ. Additional analyses and poster preparation were supported by a grant from MAP Pharmaceuticals, Mountain View, CA and Allergan Inc., Irvine, CA to the National Headache Foundation.






















