Download

1 / 25
250 likes | 489 Views
PLANNING HEALTHCARE FACILITIES for BENEFITS REALISATION Professor Keith Alexander Centre for Facilities Management Manchester, UK. PLANNING HEALTHCARE FACILITIES for BENEFITS REALISATION Benefits realisation Community Health Partnerships Healthy communities Case study – Bolton One

E N D
PLANNING HEALTHCARE FACILITIES for BENEFITS REALISATIONProfessor Keith AlexanderCentre for Facilities ManagementManchester, UK
PLANNING HEALTHCARE FACILITIES for BENEFITS REALISATION Benefits realisation Community Health Partnerships Healthy communities Case study – Bolton One Community-based Facilities Management
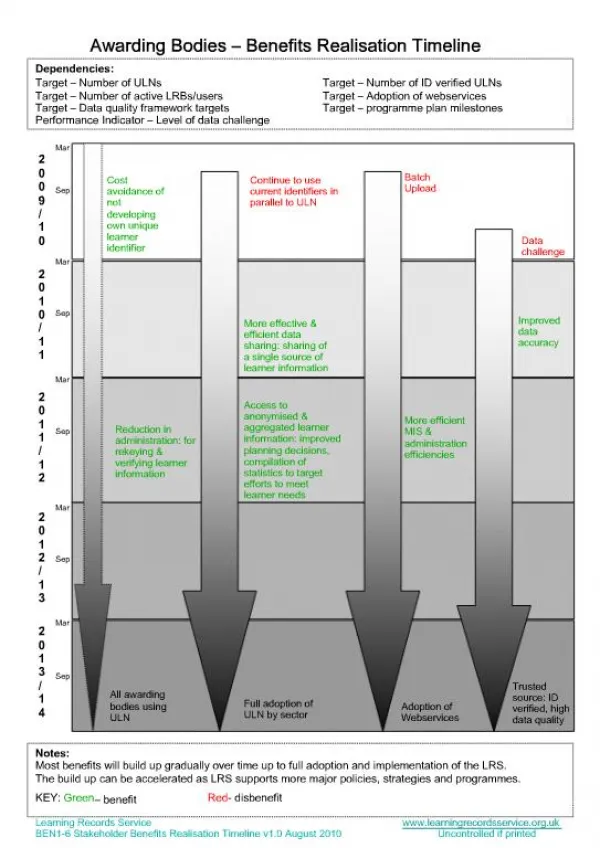
BENEFITS REALISATION Programme and project Projects deliver products Programmes deliver outcomes Benefits realisation fills the gap between the two Projects are measured in terms of their achievement of objectives within budget, within the required time frames and at the requisite levels of quality but, very often achieving all these criteria results in the overall organisational benefits not being met.
BENEFITS REALISATION ‘The processes of planning and managing a programme or project so that potential benefits to all stakeholders, arising from organisational transformation, are actually achieved’ (Alexander 2009) Public service/social benefit Social return on investment (SROI) • What is the benefit? • Which strategic objective does the benefit • support? • When is the benefit expected to accrue? • On what enablers or changes does the benefit rely? • Which stakeholders own the benefit and which receive it? • How is it measured and tracked? Benefits profile Benefits realisation plan Evaluation/reviews Change and benefits Benefits management strategy l High level benefits map Keith – great if you would take a ‘planning change’ perspective – approximately 5 to 7 slides maximum? BeReal 9
Feedforward Built environment ACTION Integrated service Health Estate Healthcare Setting (Healthscape) Service User Experience Healthcare (outcomes) Value chain Hotel services REFLECTION Non clinical support Feedback HEALTHCARE FACILITIES MANAGEMENT WP 6 – Facilities and service management and use
COMMUNITY HEALTH PARTNERSHIPS ‘Innovative and creative solutions to procure and develop assets that enhance health and social care provision’ Local Improvement Finance Trust (LIFT) PPP model Integration of health and social care services Regeneration objectives
COMMUNITY HEALTH PARTNERSHIPS ‘Delivering Healthy Communities through Partnership’
NHS PLAN 2000 The NHS will enter into a new public private partnership within a new equity stake company – the NHS Local Improvement Finance Trust (NHS Lift) – to improve primary care premises in England. Up to £1 billion will be invested in primary care facilities The investment will allow for a range of brand new types of NHS facilities, bringing primary and community services – and where possible social services – together under one roof to make access more convenient for patients. New one-stop primary care centres will include GPs, dentists, opticians, health visitors, pharmacists and social workers.
LIFT PROGRAMME Service led initiative to bring about radical change in primary and social care Bring new capital investment into Primary Care Seeking to co-locate integrated health & social care services and facilities Long term partnership involving: Local health and social care economy 20% Private Sector Partner (PSP) 60% Community Health partnerships 20%
STRATEGIC CONTEXT Improve access to public services Tackle health inequalities Improve level of health and well being Shift of care from hospitals to the community Hospital building programme – capacity assumptions Good health is not solely the remit of the health service – integration of public sector community services Primary care estate condition and suitability particularly in deprived areas Traditional lease leaves risk with clinicians
STRATEGIC CONTEXT Need For: Integrated community based care facilities and services determined by local requirements and an efficient delivery mechanism. Integration and shift in services between Primary / Intermediate / Secondary / Local Authority services, Voluntary Sector etc Recruitment and retention of clinicians and staff in deprived areas.
LIFT PROGRAMME Partnership establishes limited companies Shareholders - LHE (20%), PfH (20%) & PSP (60%) LIFTCo becomes strategic partner for locality Plan, design, build/refurbish & maintain primary & social care premises Assets owned by LIFTCo and rented to health and social care providers Provides a range of partnering services to support public sector Brings a commerciality to service and premises decisions
LIFT PROGRAMME The intended benefits Improvements in healthcare outcomes; Broader, more complex range of services in areas of greatest need; Improved accessibility of the healthcare system; Integration of health and social care; Faster, more referrals; Flexibility to changing requirements; Additional community facilities; Improved usability Viability; Sustainability;
CMI Action Cluster Meeting St Peter’s Health and Leisure Centre Burnley, Friday 29 March 2008 SUSTAINABLE FACILITIES Promoting health and well-being PCT leadership in sustainability LIFT and regeneration Regeneration outcomes
CONCLUSIONS Evidence base – achievement, engagement, impact, footprint Build customer intelligence Opportunities – health promotion, community enterprise Is co-location enough? Develop partnership working
BRAHM LIFT Bolton, Rochdale and Heywood and Middleton LIFT Formed in 2007 NHS Bolton, NHS HMR and Eric Wright Group Strategic Partnership Board Bolton One Bolton PCT, Bolton Council, University of Bolton
INTEGRATED FACILITIES • Health • urgent care facilities • primary care facilities • diagnostics • specialised, community-based treatment • Leisure • 8-lane 25m swimming pool – with movable floor • hydro-therapy pool • fitness suite • access to University sports facilities • Teaching and research • clinical skills laboratory facilities • a rehabilitation suite, including rehabilitation clinics • sports injury and exercise and conditioning clinics • a test-running track
NHS CORPORATE CITIZENSHIP Service Patient Experience Learning Usability Workplace appraisal Community Social Local employment and training Community engagement Local impact (LM3) Assets Procurement Supplier diversity 5 PERSPECTIVES Environmental Environmental sustainability Carbon reduction commitment (10:10) BREEAM: Healthcare XB COMMUNITY BASED FACILITIES MANAGEMENT