Download
1 / 40
450 likes | 1.29k Views
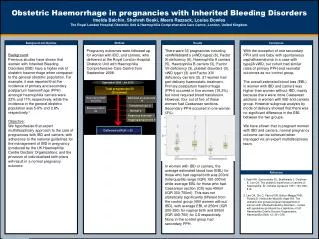
Obstetric haemorrhage. ESMOE. Aims. To recognise obstetric haemorrhage To understand the causes of haemorrhage To practise the skills needed to respond to a woman who is bleeding To achieve competence in those skills. Haemorrhage is Common. Most common cause of maternal death worldwide

E N D
Obstetric haemorrhage ESMOE
Aims • To recognise obstetric haemorrhage • To understand the causes of haemorrhage • To practise the skills needed to respond to a woman who is bleeding • To achieve competence in those skills
Haemorrhage is Common • Most common cause of maternal death worldwide • Accounts for ~30% of maternal deaths • Deaths from haemorrhage could often beavoided. (In RSA, over 80% of haemorrhage deaths are avoidable)
Prevention of Haemorrhage • Routine iron supplementation in pregnancy • Anticipate / be prepared • Detect women at risk and deliver at referral hospital • Available supplies - IV fluids, cannulae, oxytocics, misoprostol, internal tamponade, blood transfusion services • Prevent prolonged labour (use of the partogram) • Active management of third stage of labour • Routine postpartum and post caesarean section monitoring of vital signs and bleeding. Use Early Warning Chart (EWC)
Haemorrhage is Often Not Recognized • Blood loss is underestimated because in pregnancy signs of hypovolaemia do not show until the losses are large • Mother can lose up to 35% of circulating blood volume (2000 mls) before showing clinical signs of hypovolaemia
Haemorrhage – Signs • Pale • Confused • Increased HR, reduced BP (late sign) • FH abnormalities • Reduced urine output • Obvious or hidden bleeding
WHEN THE SIGNS ARE THERE, THEY ARE SIGNIFICANT, SO DO NOT IGNORE THEM AND ACT QUICKLY
All Cases of Haemorrhage Call-a-C A B Circulation IV access by 2 large bore canulae Send off blood samples Give iv fluids and blood if available Catheterise the patient and monitor output Be aware of potential coagulation disorders
Antepartum Haemorrhage (APH) Abruptio placentae Placenta praevia APH of unknown origin (APHUO)
Abruptio Placentae Is a clinical diagnosis Signs: • Tender tense enlarged uterus • Degree of shock not always proportional to revealed blood loss • Fetal distress or demise and can develop complications – renal failure, clotting problems and anticipate a PPH
Abruptio Placentae- Management Call-a-CAB! Resuscitate Make a diagnosis Control the bleeding Mx is delivery
Live Baby Rupture membranes Resuscitate mother and as soon as stable emergency delivery Dead Baby Resuscitate mother and induce labour by rupture of membranes Refer immediately Management Abruptio Placentae
Placenta Praevia (PP) All other APHs must undergo ultrasound to exclude PP All PPs must be referred It is essential that the most senior surgeon performs any surgery It is advisable to have some form of tamponade available at surgery
APHUO PV bleed in the absence of placenta praevia, abruptio or local causes Danger – atypical abruptio (50%) Refer Mx: admit for 6 hourly CTG Earliest sign of abruptio – spont decels → immediate CD
Haemorrhage - Management Call-a-CAB! Resuscitate Control the bleeding Make a diagnosis Treat!
Approach – After Vaginal Delivery • Is the uterus contracted? • If not – atony or retained products • Contract the uterus • Is the uterus empty? • If not – empty the uterus • The uterus is contracted? • Trauma – find site • Is the uterus there? • No = uterine inversion – correct stat
Uterine Atony • Massage uterus / bimanual compression • Give oxytocics (oxytocin,ergometrine,prostaglandin) • Empty bladder • Aortic compression • Ongoing bleeding - look for other causes • Ongoing bleeding - uterine balloon tamponade • Ongoing bleeding – EUA • laparotomy • Do not delay
Bimanual Compression(Source: B-lynch. A Textbook of PPH.2006)
Rusch hydrostatic balloon catheterSource: B-Lynch, Textbook of PPH,2006.
Retained Placenta Should ideally be removed in theatre under anaesthesia If not possible or patient bleeding heavily Remove in labour ward with analgesia
Skills station : Postpartum Haemorrhage & Skills Station : Manual Removal of Placenta
Retained Placental Products Should be removed in theatre under anaesthesia First explore the uterus manually Beware of perforation with instrument use If needed – curettage with the largest curette available Uterine contraction with ↓ bleeding = empty uterus
Genital Tract Trauma Examine perineum visually Examine vagina digitally
Unknown Cause If the cause is not obvious early resort to examination under anaesthesia in theatre is essential
Observations Post-haemorrhage 1st 2 hours post-op/event: ½ hourly observations Next 4 hours: 2 hourly observations Then 4 hourly
Observations to Be Recorded Pulse rate Blood pressure Vaginal bleeding (pad checks) (Urine output and temperature)
Observations Should be performed in an area where health care professionals can do the observations regularly EARLY RECOURSE BACK TO THEATER DO NOT WAIT AND SEE!
Transfer of Unstable Patients ? • District hospital; Transfer or treat? • Importance of resuscitation measures to have been commenced and some temporising measures to arrest bleeding initiated before and continued during referral. • Temporising measures: • Uterine tamponade
Recap • Recognising Obstetric Haemorrhage • Causes • Management • Protocol • CAB • Blood replacement • Diagnosis of cause of bleeding • Methods to arrest haemorrhage