Download
1 / 1
10 likes | 135 Views
Implementing Rapid HIV Testing in Non-traditional Sites. Methods. Methods. Counselors completed a full day training session on counseling for the rapid test. NJDHSS provided a laboratory director for sites that did not have a laboratory director.

E N D
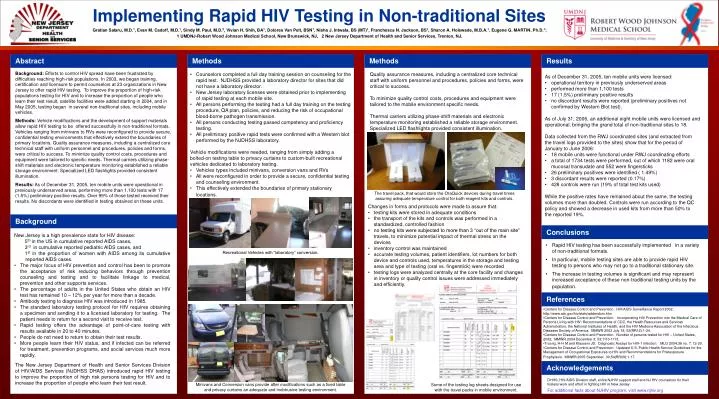
Implementing Rapid HIV Testing in Non-traditional Sites Methods Methods • Counselors completed a full day training session on counseling for the rapid test. NJDHSS provided a laboratory director for sites that did not have a laboratory director. • New Jersey laboratory licenses were obtained prior to implementing of rapid testing at each mobile site. • All persons performing the testing had a full day training on the testing procedure, QA plan, policies, and reducing the risk of occupational blood-borne pathogen transmission. • All persons conducting testing passed competency and proficiency testing. • All preliminary positive rapid tests were confirmed with a Western blot performed by the NJDHSS laboratory. • Vehicle modifications were needed, ranging from simply adding a • bolted-on testing table to privacy curtains to custom-built recreational • vehicles dedicated to laboratory testing. • Vehicles types included minivans, conversion vans and RVs • All were reconfigured in order to provide a secure, confidential testing and counseling environment. • This effectively extended the boundaries of primary stationary locations. Quality assurance measures, including a centralized core technical staff with uniform personnel and procedures, policies and forms, were critical to success. To minimize quality control costs, procedures and equipment were tailored to the mobile environment specific needs. Thermal carriers utilizing phase-shift materials and electronic temperature monitoring established a reliable storage environment. Specialized LED flashlights provided consistent illumination. The travel pack, that would store the OraQuick devices during travel times assuring adequate temperature control for both reagent kits and controls. New Jersey is a high prevalence state for HIV disease: 5th in the US in cumulative reported AIDS cases, 3rd in cumulative reported pediatric AIDS cases, and 1st in the proportion of women with AIDS among its cumulative reported AIDS cases. • The major focus of HIV prevention and control has been to promote the acceptance of risk reducing behaviors through prevention counseling and testing and to facilitate linkage to medical, prevention and other supports services. • The percentage of adults in the United States who obtain an HIV test has remained 10 – 12% per year for more than a decade. • Antibody testing to diagnose HIV was introduced in 1985. • The standard laboratory testing protocol for HIV requires obtaining a specimen and sending it to a licensed laboratory for testing. The patient needs to return for a second visit to receive test. • Rapid testing offers the advantage of point-of-care testing with results available in 20 to 40 minutes. • People do not need to return to obtain their test results. • More people learn their HIV status, and if infected can be referred for treatment, prevention programs, and social services much more rapidly. Recreational Vehicles with “laboratory” conversion. The New Jersey Department of Health and Senior Services Division of HIV/AIDS Services (NJDHSS DHAS) introduced rapid HIV testing to improve the proportion of high risk persons testing for HIV and to increase the proportion of people who learn their test result. Minivans and Conversion vans provide after modifications such as a fixed table and privacy curtains an adequate and inobtrusive testing environment. Some of the testing log sheets designed for use with the travel packs in mobile environment. Gratian Salaru, M.D.1, Evan M. Cadoff, M.D.1, Sindy M. Paul, M.D.2, Vivian H. Shih, BA1, Dolores Van Pelt, BSN1, Nisha J. Intwala, BS (MT)1, Franchesca N. Jackson, BS1, Sharon A. Holswade, M.B.A.1, Eugene G. MARTIN, Ph.D.1; 1 UMDNJ-Robert Wood Johnson Medical School, New Brunswick, NJ, 2 New Jersey Department of Health and Senior Services, Trenton, NJ. Abstract Results Background: Efforts to control HIV spread have been frustrated by difficulties reaching high-risk populations. In 2003, we began training, certification and licensure to permit counselors at 23 organizations in New Jersey to offer rapid HIV testing. To improve the proportion of high-risk populations testing for HIV and to increase the proportion of people who learn their test result, satellite facilities were added starting in 2004, and in May 2005, testing began in several non-traditional sites, including mobile vehicles. Methods: Vehicle modifications and the development of support materials allow rapid HIV testing to be offered successfully in non-traditional formats. Vehicles ranging from minivans to RVs were reconfigured to provide secure, confidential testing environments that effectively extend the boundaries of primary locations. Quality assurance measures, including a centralized core technical staff with uniform personnel and procedures, policies and forms, were critical to success. To minimize quality control costs, procedures and equipment were tailored to specific needs. Thermal carriers utilizing phase-shift materials and electronic temperature monitoring established a reliable storage environment. Specialized LED flashlights provided consistent illumination. Results: As of December 31, 2005, ten mobile units were operational in previously underserved areas, performing more than 1,100 tests with 17 (1.5%) preliminary positive results. Over 99% of those tested received their results. No discordants were identified in testing obtained on these units. • As of December 31, 2005, ten mobile units were licensed: • operational territory in previously underserved areas • performed more than 1,100 tests • 17 (1.5%) preliminary positive results • no discordant results were reported (preliminary positives not confirmed by Western Blot test). • As of July 31, 2006, an additional eight mobile units were licensed and • operational, bringing the grand total of non-traditional sites to 18. • Data collected from the RWJ coordinated sites (and extracted from • the travel logs provided to the sites) show that for the period of • January to June 2006: • 18 mobile units were functional under RWJ coordinating efforts • a total of 1734 tests were performed, out of which 1182 were oral mucosal transudate and 552 were fingersticks • 26 preliminary positives were identified ( 1.49%) • 3 discordant results were reported (0.17%) • 428 controls were run (19% of total test kits used) • While the positive rates have remained about the same, the testing • volumes more than doubled. Controls were run according to the QC • policy and showed a decrease in used kits from more than 50% to • the reported 19%. • Changes in forms and protocols were made to assure that: • testing kits were stored in adequate conditions • the transport of the kits and controls was performed in a standardized, controlled fashion • no testing kits were subjected to more than 3 “out of the main site” travels, to minimize potential impact of thermal stress on the devices • inventory control was maintained • accurate testing volumes, patient identifiers, lot numbers for both device and controls used, temperatures in the storage and testing area and type of testing (oral vs. fingerstick) were recorded • testing logs were analyzed centrally at the core facility and changes in inventory or quality control issues were addressed immediately and efficiently. Background Conclusions • Rapid HIV testing has been successfully implemented in a variety of non-traditional formats. • In particular, mobile testing sites are able to provide rapid HIV testing to persons who may not go to a traditional stationary site. • The increase in testing volumes is significant and may represent increased acceptance of these non-traditional testing units by the population. References • Centers for Disease Control and Prevention. HIV/AIDS Surveillance Report 2002. http://www.cdc.gov/hiv/stats/addendum.htm • Centers for Disease Control and Prevention. Incorporating HIV Prevention into the Medical Care of Persons Living with HIV: Recommendations of CDC, the Health Resources and Services Administration, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR 2003 July 18; 52(RR12):1-24. • Centers for Disease Control and Prevention. Number of persons tested for HIV – United States, 2002. MMWR 2004 December 3; 53:1110-1113. • Truong, H-H M and Klausenr JD. Diagnostic Assays for HIV-1 infection. MLO 2004;36 no. 7: 12-20. • Centers for Disease Control and Prevention. Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HIV and Recommendations for Postexposure Prophylaxis. MMWR 2005 September 30;54(RR09):1-17. Acknowledgements DHHS, HIV/AIDS Division staff, entire NJHIV support staff and NJ HIV counselors for their tireless work and effort in fighting HIV in New Jersey For additional facts about NJHIV program, visit www.njhiv.org