Download
1 / 74
810 likes | 1.12k Views
Evaluation & Treatment of Urinary Incontinence. Andy M. Norman, M.D. Assistant Clinical Professor, Ob- Gyn Vanderbilt University Medical Center. Goals. Discuss Urinary Incontinence (UI) Discuss Incidental Causes of UI DIAPERS Mnemonic Discuss Preliminary Diagnostics

E N D
Evaluation & Treatment of Urinary Incontinence Andy M. Norman, M.D. Assistant Clinical Professor, Ob-Gyn Vanderbilt University Medical Center
Goals • Discuss Urinary Incontinence (UI) • Discuss Incidental Causes of UI • DIAPERS Mnemonic • Discuss Preliminary Diagnostics • Discuss Treatment of Urgency UI • Discuss Treatment of Stress UI • Discuss Overflow Incontinence • Review Some Cases of UI with Emphasis on Medical Management
Acknowledgement • Cases designed by: Dr. Patricia Goode, IM/Geriatrics, UAB • Special thanks to: Kathryn Burgio, PhD, UAB • Author of “Staying Dry,” a self help book for patients incontinence.
Disclaimer I am a Urogynaecologist. All of my incontinence patients are female. This discussion is, therefore, mostly centered around problems of females. Some of the observations and treatments are also applicable to male patients.
Prevalence of Urinary Incontinence • Age 15 to 64 1.5 - 5% men 10-30% women • Noninstitutionalized 15-35%>60 years old Twice as high in women • Homebound elderly 50% • Nursing home residents 50% (two thirds if catheterized population included)
In 1995, more than $16.3 billion was spent on urinary incontinence care. More is spent on incontinence care than other chronic diseases such as breast cancer and osteoporosis.
ICS DEFINITION OF URINARY INCONTINENCE Complaint of any involuntary leakage of urine International Continence Society.Abrams P, et al. Neurourol Urodyn. 2002;21(2):167-178.
Urinary Incontinence Transient Causes of Incontinence Urge Incontinence Stress Urinary Incontinence Mixed Incontinence Both Urgency & Stress Induced Overflow Incontinence
URINARY INCONTINENCE 3884 community-dwelling older adult volunteers for a health promotion study Ages 65 – 79 1104 (28.4%) had self-reported incontinence Burgio, et al: JAGS 42: 208, 1994 Treatment Seeking (1)
URINARY INCONTINENCE Treatment Seeking (2) % reporting to M.D. Burgio et al: JAGS 42: 208, 1994
URINARY INCONTINENCE Personal problem (not medical) Embarrassed Normal after childbearing Normal aging change Fear of nursing home placement Afraid treatment requires surgery Failure to Report UI to Health Care Provider
INCONTINENCE YOU GOTTA ASK!!
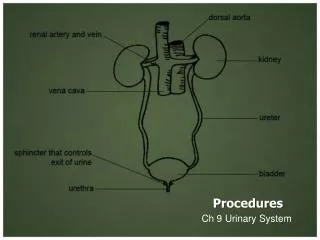
Diagnosis of UI • History • Physical Exam • Pelvic Organ Prolapse Assessment • In & Out Cath for Residual Urine Volume • U/A +/- Urine C & S • Qtip Test for Bladder Neck Hypermobility
BLADDER DIARY Fluid intake Time, type, amount Urine output Time, amount Urine leakage Time, amount Precipitating events (cough, sneeze, exercise, etc.) Associated symptoms (urgency, pain, etc.) Pad usage Number, type
Transient Causes of UI • Drugs & Diet • Infection • Atrophic Urethritis • Psychological - Depression, Delirium • Endocrine - Diabetes, Hypercalcemia • Restricted Mobility • Stool Impaction
Transient Causes of UI • DRUGS • ACE Inhibitors -- cough • Alpha Blockers – relax internal sphincter • Anticholinergics/Antimuscularinics – decrease effective bladder emptying • Diuretics -- timing • Neuroleptics – pseudoparkinsonism • Sedatives – especially in the demented • DIET • Caffeine – provokes detrusor instability • Artificial Sweeteners-bladder irritants
Urgency Incontinence(Overactive Bladder) Therapeutic Options
Behavioral Treatment: Multi-component Programs Pelvic floor muscle training Home practice and exercise Self-Monitoring Voiding schedules—timed and prompted voiding “Urge” strategies—FREEZE & SQUEEZE
Biofeedback Teaching method Facilitates learned control of physiological responses Patients learn by feedback of their attempts to control bladder and sphincter responses.
Detrusor Contraction 10 mmHg
When the Urge Strikes“Freeze & Squeeze” Stop and stay still Squeeze pelvic floor muscles Relax rest of body Concentrate on suppressing urge Wait until the urge subsides Walk to bathroom at normal pace
When to Void WorstTime WorstTime BestTime CalmPeriod
RCT Comparing Behavior and Drug Therapy 197 older, community-dwelling women with Urge Incontinence Randomized to: Behavioral training (biofeedback) Drug therapy (oxybutynin) Placebo control Burgio et al, JAMA, 1998
Biofeedback-Assisted Behavioral Treatment Visit #1: Anorectal BF to teach PFM control. Home exercise instructions. Visit #2: “Urge strategies” and “stress strategies” Visit #3: If not >50% improved, bladder/sphincter biofeedback Visit #4: Individual adjustments and reinforcement
Reduction of Incontinencein the Randomized Clinical Trial % Reduction
Patient Satisfaction with Treatment for Urge Urinary Incontinence
Behavioral Training Tested the same behavioral program with all components minus biofeedback vs. Verbal feedback based on Vaginal Palpation vs. Same program, but Booklet form (Minimal Treatment Control). Is Biofeedback a necessary component? Burgio, Goode, et.al., JAMA, 2002
Reduction of Incontinencein a Randomized Clinical Trial % Reduction Burgio, Goode, et.al., JAMA, 2002
Stress urinary incontinence is the most common type of incontinence in women Burgio, Matthews and Engel, 1991
Stress incontinence = Urethral incompetenceBladder Neck Hypermobility Intrinsic Sphincter Deficiency Pelvic Organ Prolapse
Treatments for SUI • Pelvic Floor Physical Therapy • Topical Estrogen Therapy • Urethral Plugs • Incontinence Pessaries • Surgical Therapy
Women’s lifetime risk of surgery for SUI or POP is 11% Olsen, Smith and Bergstrom, 1997
TVT – Transvaginal Tape • Relatively new procedure • Large cohort analysis shows cure rate 80%, improvement 94% • Kuuva, 2000
CONCLUSIONS regards Surgical Care of SUI • Numerous surgical techniques to treat stress incontinence • Important to know both objective and subjective cure rates as well as side effects of surgical procedures • Thoughtful evaluation of patients with individualization of therapy is advisable
Overflow Incontinence • Common Causes • Obstuctive Uropathy such as BPH in men and Pelvic Organ Prolapse in women. • Neurogenic Bladder • Treatments • Relief of the Obstruction • Clean Intermittent Self Catheterization • Indwelling Catheters • Diversion Procedures
SUMMARY Incontinence is very common, so question ALL patients Reversible causes of UI D – I – A – P – E – R – S Behavioral Therapy Effective No side effects
Transient Causes of UI • Drugs & Diet • Infection • Atrophic Urethritis • Psychological - Depression, Delirium • Endocrine - Diabetes, Hypercalcemia • Restricted Mobility • Stool Impaction Try with Some Case Studies
PATIENT CASE 1 48 year old woman Complains that she just can’t get to the bathroom fast enough for the past 3 months 1-2 urge accidents per day (no stress) Nocturia x 2, often with an accident Wears a pad all the time Wants a bladder tack History
PATIENT CASE 1 Last menstrual period 6 months ago Having hot flashes Afraid to take hormone replacement therapy Trying to lose weight; drinks 6-8 diet Cokes per day History
PATIENT CASE 1 EXAM Vaginal mucosa mildly atrophic Otherwise exam normal URINALYSIS Normal PVR 40 cc
PATIENT CASE 1 Drugs & Diet Caffiene Taper off caffeine ½ per week Begin Exercising Infection Atrophic Urethritis Yes Consider HRT Vaginal estrogen cream – ½ gram 3 times/week to vaginal entrance
PATIENT CASE 1 Psychological - no Endocrine - no Restricted Mobility – no Stool Impaction – no
PATIENT CASE 1 Taper off Caffeine Vaginal Estrogen Drugs? Hold off for now Behavioral Training TREATMENT
PATIENT CASE 1 Teach Kegel exercises during her exam Home Exercises 10 paired contractions and relaxations 3 seconds each – build up to 10 seconds TID (standing, sitting, lying) Urge Strategy Freeze/Squeeze to suppress urgency RTC 1 month Behavioral Treatment