Download
1 / 1
10 likes | 93 Views
HIV CENTER for Clinical and Behavioral Studies. Mixed/ Other 6%. White 50%. Hispanic 25%. Black 13%. API 6%. Single / never married 62%. Committed 28%. Other 6%. DP/CU 3%. Homosexual/Gay 81%. Heterosex’l 13%. Bisex’l 6%. 1.34. 2.50. 2.57. HIV+ partners. 3.75. 0.66.

E N D
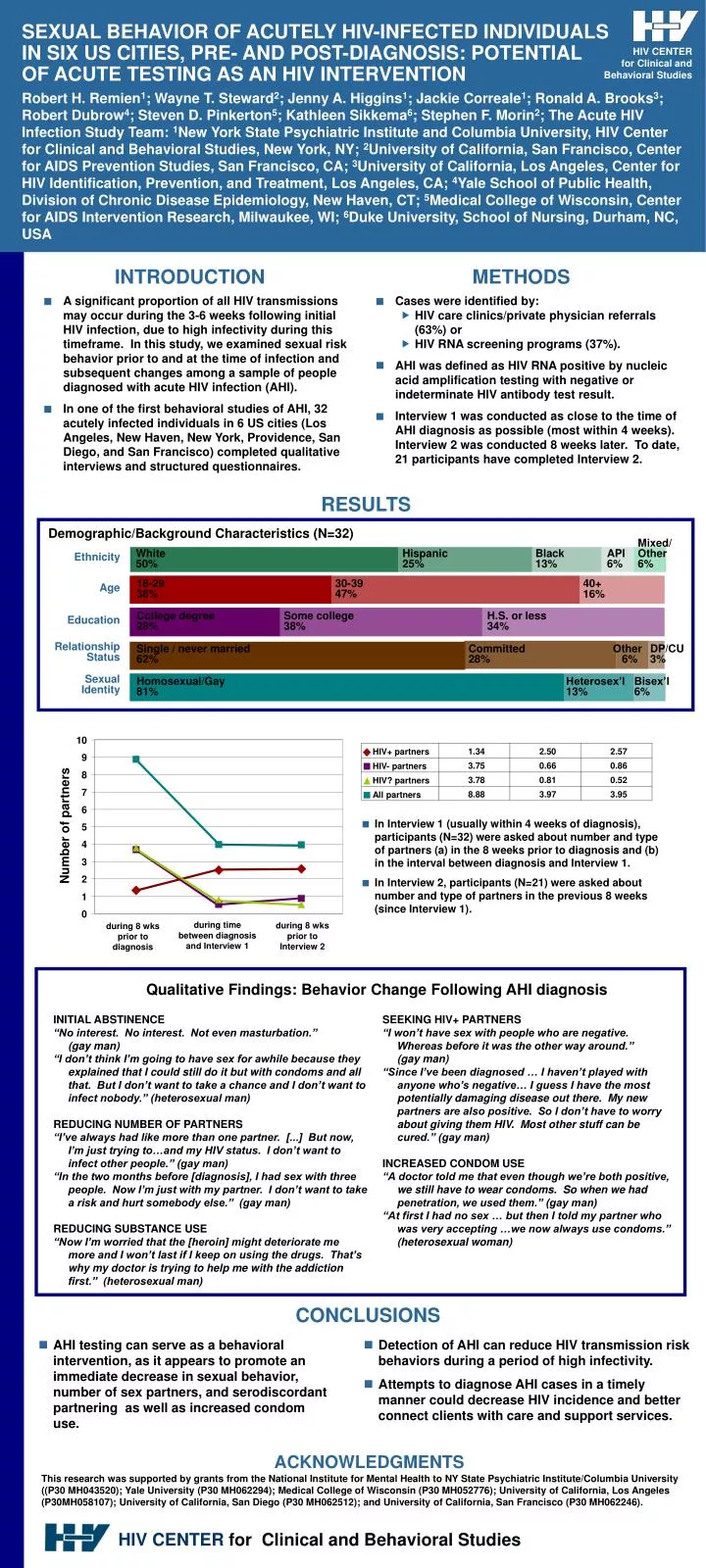
HIV CENTER for Clinical and Behavioral Studies Mixed/ Other6% White50% Hispanic 25% Black13% API 6% Single / never married 62% Committed28% Other 6% DP/CU 3% Homosexual/Gay81% Heterosex’l13% Bisex’l 6% 1.34 2.50 2.57 HIV+ partners 3.75 0.66 0.86 HIV- partners 3.78 0.81 0.52 HIV? partners 8.88 3.97 3.95 All partners SEXUAL BEHAVIOR OF ACUTELY HIV-INFECTED INDIVIDUALS IN SIX US CITIES, PRE- AND POST-DIAGNOSIS: POTENTIAL OF ACUTE TESTING AS AN HIV INTERVENTION Robert H. Remien1; Wayne T. Steward2; Jenny A. Higgins1; Jackie Correale1; Ronald A. Brooks3; Robert Dubrow4; Steven D. Pinkerton5; Kathleen Sikkema6; Stephen F. Morin2; The Acute HIV Infection Study Team: 1New York State Psychiatric Institute and Columbia University, HIV Center for Clinical and Behavioral Studies, New York, NY; 2University of California, San Francisco, Center for AIDS Prevention Studies, San Francisco, CA; 3University of California, Los Angeles, Center for HIV Identification, Prevention, and Treatment, Los Angeles, CA; 4Yale School of Public Health, Division of Chronic Disease Epidemiology, New Haven, CT; 5Medical College of Wisconsin, Center for AIDS Intervention Research, Milwaukee, WI; 6Duke University, School of Nursing, Durham, NC, USA INTRODUCTION METHODS • A significant proportion of all HIV transmissions may occur during the 3-6 weeks following initial HIV infection, due to high infectivity during this timeframe. In this study, we examined sexual risk behavior prior to and at the time of infection and subsequent changes among a sample of people diagnosed with acute HIV infection (AHI). • In one of the first behavioral studies of AHI, 32 acutely infected individuals in 6 US cities (Los Angeles, New Haven, New York, Providence, San Diego, and San Francisco) completed qualitative interviews and structured questionnaires. • Cases were identified by: • HIV care clinics/private physician referrals (63%) or • HIV RNA screening programs (37%). • AHI was defined as HIV RNA positive by nucleic acid amplification testing with negative or indeterminate HIV antibody test result. • Interview 1 was conducted as close to the time of AHI diagnosis as possible (most within 4 weeks). Interview 2 was conducted 8 weeks later. To date, 21 participants have completed Interview 2. RESULTS Demographic/Background Characteristics (N=32) Ethnicity 18-2938% 30-3947% 40+16% Age College degree28% Some college38% H.S. or less34% Education Relationship Status Sexual Identity 10 9 8 7 6 • In Interview 1 (usually within 4 weeks of diagnosis), participants (N=32) were asked about number and type of partners (a) in the 8 weeks prior to diagnosis and (b) in the interval between diagnosis and Interview 1. • In Interview 2, participants (N=21) were asked about number and type of partners in the previous 8 weeks (since Interview 1). Number of partners 5 4 3 2 1 0 during time between diagnosis and Interview 1 during 8 wks prior to Interview 2 during 8 wks prior to diagnosis Qualitative Findings: Behavior Change Following AHI diagnosis INITIAL ABSTINENCE “No interest. No interest. Not even masturbation.” (gay man) “I don’t think I’m going to have sex for awhile because they explained that I could still do it but with condoms and all that. But I don’t want to take a chance and I don’t want to infect nobody.” (heterosexual man) REDUCING NUMBER OF PARTNERS “I’ve always had like more than one partner. [...] But now, I’m just trying to…and my HIV status. I don’t want to infect other people.” (gay man) “In the two months before [diagnosis], I had sex with three people. Now I’m just with my partner. I don’t want to take a risk and hurt somebody else.” (gay man) REDUCING SUBSTANCE USE “Now I’m worried that the [heroin] might deteriorate me more and I won’t last if I keep on using the drugs. That’s why my doctor is trying to help me with the addiction first.” (heterosexual man) SEEKING HIV+ PARTNERS “I won’t have sex with people who are negative. Whereas before it was the other way around.” (gay man) “Since I’ve been diagnosed … I haven’t played with anyone who’s negative… I guess I have the most potentially damaging disease out there. My new partners are also positive. So I don’t have to worry about giving them HIV. Most other stuff can be cured.” (gay man) INCREASED CONDOM USE “A doctor told me that even though we’re both positive, we still have to wear condoms. So when we had penetration, we used them.” (gay man) “At first I had no sex … but then I told my partner who was very accepting …we now always use condoms.” (heterosexual woman) CONCLUSIONS • AHI testing can serve as a behavioral intervention, as it appears to promote an immediate decrease in sexual behavior, number of sex partners, and serodiscordant partnering as well as increased condom use. • Detection of AHI can reduce HIV transmission risk behaviors during a period of high infectivity. • Attempts to diagnose AHI cases in a timely manner could decrease HIV incidence and better connect clients with care and support services. ACKNOWLEDGMENTS This research was supported by grants from the National Institute for Mental Health to NY State Psychiatric Institute/Columbia University ((P30 MH043520); Yale University (P30 MH062294); Medical College of Wisconsin (P30 MH052776); University of California, Los Angeles (P30MH058107); University of California, San Diego (P30 MH062512); and University of California, San Francisco (P30 MH062246).






