Download
1 / 52
550 likes | 696 Views
Newer modes of ventilation. Dr P K Dash Trivandrum. Transition. Older ventilators. Newer ventilators. History of ventilation. Introduction of modes. Goals of ventilation. Best mode selection. Why new modes. More safely assist patient

E N D
Newer modes of ventilation Dr P K Dash Trivandrum
Why new modes • More safely assist patient • Less likelihood of ventilator associated lung injury. • Less hemodynamic compromise • More effectively ventilate/oxygenate • Improve patient - ventilator synchrony • More rapid weaning
Evolution • Volume control • Pressure control • Pressure support • Dual control • Algorithm based • Knowledge based
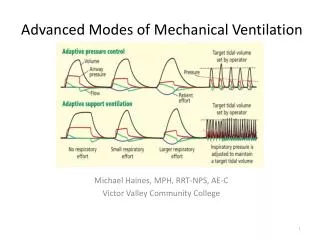
Newer modes • Dual control modes • Proportional Assist Ventilation (PAV) • Closed loop PSV • Automatic tube compensation • Adaptive Support Ventilation (ASV)
First generation dual modesVAPS and PA • Combines volume ventilation & pressure support • Uses TV, peak flow, and pressure support • Targets PS level with at least set peak flow • Continues until flow decreases to set peak flow, then: • If TV not delivered, peak flow maintained until vol. limit • If TV or more delivered, breath ends Bear 1000 Bird 8400Sti Tbird
First generation dual modesPRVC and Volume support • Combines volume ventilation & pressure control • Set TV is “targeted” • Ventilator estimates vol./press. relationship each breath • Ventilator adjusts level of pressure control breath by breath Servo 300 Maquet Servo-i
PRVC • Test breath (5 cm H2O); • Pressure is increased to deliver set volume; • Maximum available pressure; • Breath delivered at preset E, at preset f, and during preset TI; (5)When VT corresponds to set value, pressure remains constant; (6) If preset volume increases, pressure decreases; the ventilator continually monitors and adapts to the patient’s needs
Volume support (1) VS test breath (5 cm H2O); (2) Pressure is increased slowly until target volume is achieved; (3) Maximum available pressure is 5 cm H2O below upper pressure limit; (4) VT higher than set VT delivered results in lower pressure; (5) Patient can trigger breath; (6) If apnea alarm is detected, ventilator switches to PRVC
Ventilator settings • Minimum respiratory rate • Target tidal volume • Upper pressure limit • FIO2 • Inspiratory time or I:E ratio • Rise time • PEEP
Advantages and disadvantages • Decelerating inspiratory flow pattern • Pressure automatically adjusted for changes in compliance and resistance within a set range • Tidal volume guaranteed • Limits volutrauma • Prevents hypoventilation • Pressure delivered is dependent on tidal volume achieved on last breath • Intermittent patient effort variable VT • Less suitable for patients with asthma or COPD
Second generation of dual modes Auto flow Evita 4, Adaptive support ventilation Hamilton Galileo
Autoflow • First breath uses set TV & I-time • Pplateau measured • Pplateau then used • V/P measured each breath • Press. changed if needed (+/- 3) • Then similar to PRVC • Adds high TV alarm & limit • Can be used in CMV, SIMV and MMV
Bi-level ventilation methodsAllow spontaneous breaths at two airway pressures • Reduction of shunt due to the alveolar recruitment • Better venous return • Reduced Risk of Pulmonary Muscle Atrophy • Weaning is enhanced Advantages of spontaneous ventilation • BiPAP (Drager E-4 & E-2 dura) • BiLevel (NPB 840) • APRV (NPB 840, Drager E-4 & E-2 dura)
BiPAP (Drager E-4 & E-2 dura) • Reduction of the invasivness of Ventilation • Reduction of Sedation • One Ventilation Mode from Intubation to Weaning • More comfortable for the Patient • Fewer Alarms (easier handling) Spontaneous Breathing BIPAP PCV
Other newer modes • Proportional assist ventilation • Smart care • Automatic tube compensation • Neural adjusted ventilator assist
Proportional assist ventilation • Supports according to the patient's effort, based on the respiratory flow signal and by adjusting inspiratory airway pressure in proportion to the patient's effort; • PAV requires accurate, instantaneous measurement of compliance and resistance • Only provides assisted ventilation • Improves patient – ventilator synchrony • Does not improve ventilation/oxygenation – no control of ventilatory pattern! • May prevent lung injury, Not shown to improve weaning!
Automatic tube compensation • Designed to Maintain Tracheal Pressure at Baseline • Does not require ongoing assessment of resistance! • Pressure Applied Based Upon Resistive Properties of the Airway and Patients Inspiratory Flow • Positive Pressure During Inspiration • Negative Pressure During Exhalation • Effectively unloads resistive effort imposed by ETT • Improves patient – ventilator synchrony • Reduces risk of lung injury • Does not improve ventilation/oxygenation – • No control over ventilatory pattern • No demonstrated improvement in weaning!
Smart care • It is a knowledge based automated weaning system. • It contains an automated clinical weaning guideline • Based on recognised medical expertise and research.
Smart care working principles • Step 1: Stabilizing within a respiratory comfort zone • Step 2: Reducing invasiveness • Step 3: Testing readiness for extubation
Level of PS is automatically adjusted in steps of 2-4 mbar to keep parameters within following ranges Spontaneous breathing rate >15 bpm<30 bpm (<34 bpm for patients with respiratory failure due to neurological disorders) Expired tidal volume >250 ml (ideal body weight <55 kg)>300 ml (ideal body weight >55 kg) End tidal CO2 <55 mmHg (<65 mmHg for patients with COPD Respiratory Comfort Zone
Neural adjusted ventilator assistNAVA Ideal Technology Central Nervous System Phrenic Nerve Diaphragm Excitation Diaphragm Contraction Chest Wall and Lung Expansion Airway Pressure, Flow and Volume New Technology Ventilator Unit Neuro-Ventilatory Coupling Current Technology
Conventional triggering Conventional ventilator technology uses a pressure drop or flow reversal to provide assistance to the patient. This is the last step of the signal chain leading to inhalation. This last step is subject to disturbances such as intrinsic PEEP, hyperinflation and leakage.
NAVA triggering • The earliest signal that can be registered with a low degree of invasivity is the excitation of the diaphragm. • The excitation of the diaphragm is independent of pneumatic influence and insensitive to the problems with pneumatic triggering technologies. • By following diaphragm excitation and adjusting the support level in synchrony with the rise and fall of the electrical discharge, the ventilator and the diaphragm will work with the same signal input. • In effect, this allows the ventilator to function as an extra muscle, unloading extra respiratory work induced by the disease process.
Signal capture • All muscles (including the diaphragm and other respiratory muscles) generate electrical activity to excite muscle contraction. • The electrical activity of the diaphragm is captured by an esophageal catheter with an attached electrode array. The signal is filtered in several steps and provide the input for control of the respiratory assist delivered by the ventilator.
Catheter verification P and QRS waves are present on the top leads and the P-waves disappear on the lower leads and with a decrease of the QRS-amplitude on the lower leads. When an Edi waveform is present, observe which leads are highlighted in blue. If the leads highlighted in blue are in the center (i.e. second and third leads), secure the Edi Catheter in this position. To finally verify correct positioning of the Edi Catheter press the Exp. Hold and keep the button depressed until a breathing effort is registered. A negative deflection in the pressure curve with a simultaneous positive inflection in the Edi curve verifies correct position of the Edi Catheter.
Setting the NAVA level NAVA preview is a help tool to set the NAVA level to reach an estimated NAVA On the uppermost waveform (the pressure curve), there are two curves presented simultaneously. The gray curve shows the estimated pressure, Pest, based on the Edi signal and the set NAVA level. NAVA preview is available in all invasive modes of ventilation except NAVA.
Post extubation monitoring Monitoring of the ventilatory pattern of the patient is superior with NAVA as the control signal of the respiratory center is known. This can of course be done in any mode of ventilation and is an invaluable tool in determining adaptation to the ventilator strategy. However, patients breathing spontaneously can also be monitored, which is a very helpful tool if patients are developing wheezing after extubation or during a T-piece trial.