Download
1 / 1
10 likes | 169 Views
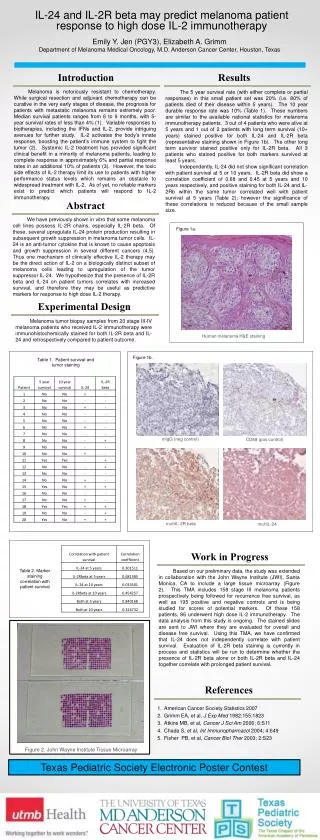
After IRB approval, this was a prospective study, done in NICU at UTMB, Galveston. Infants (30-36 weeks) requiring PHT for NH were included & infants with congenital anomalies of GI tract (could affect NH) were excluded. All management decisions of NH were taken by the neonatal attending.

E N D
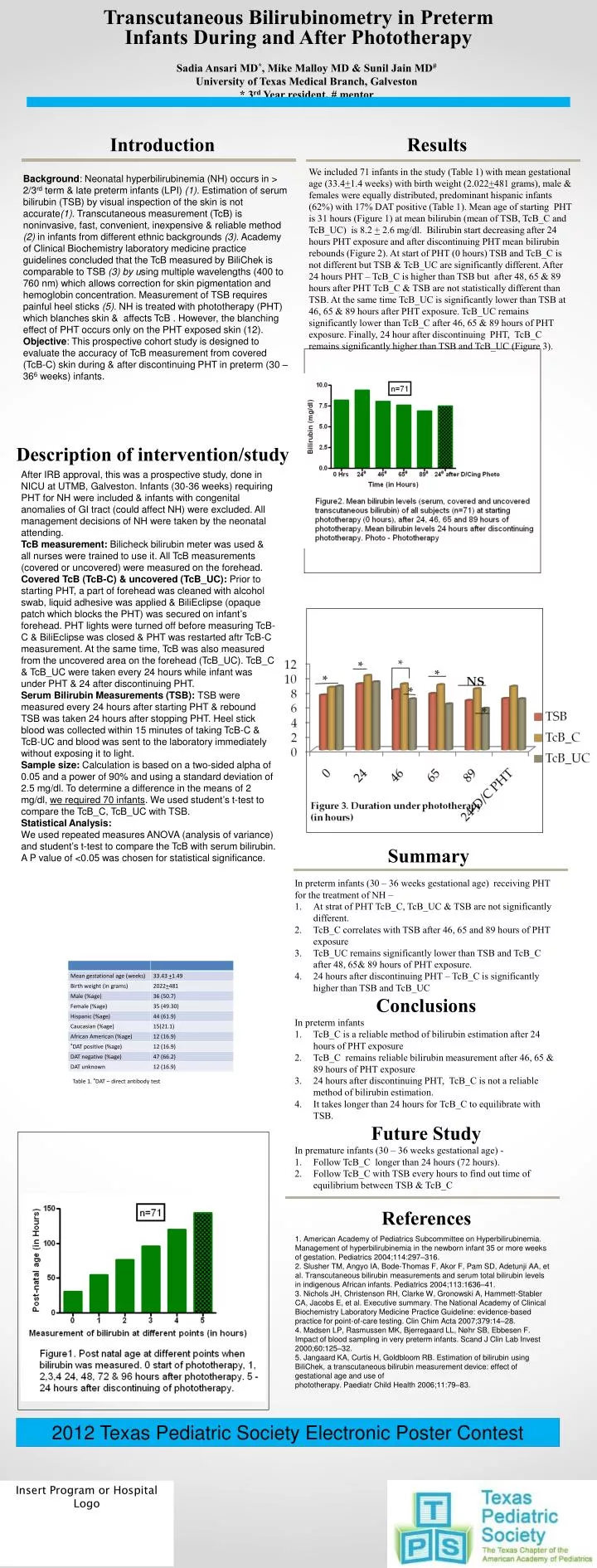
After IRB approval, this was a prospective study, done in NICU at UTMB, Galveston. Infants (30-36 weeks) requiring PHT for NH were included & infants with congenital anomalies of GI tract (could affect NH) were excluded. All management decisions of NH were taken by the neonatal attending. TcB measurement: Bilicheck bilirubin meter was used & all nurses were trained to use it. All TcB measurements (covered or uncovered) were measured on the forehead. Covered TcB (TcB-C) & uncovered (TcB_UC): Prior to starting PHT, a part of forehead was cleaned with alcohol swab, liquid adhesive was applied & BiliEclipse (opaque patch which blocks the PHT) was secured on infant’s forehead. PHT lights were turned off before measuring TcB-C & BiliEclipse was closed & PHT was restarted aftr TcB-C measurement. At the same time, TcB was also measured from the uncovered area on the forehead (TcB_UC). TcB_C & TcB_UC were taken every 24 hours while infant was under PHT & 24 after discontinuing PHT. Serum Bilirubin Measurements (TSB): TSBwere measured every 24 hours after starting PHT & rebound TSB was taken 24 hours after stopping PHT. Heel stick blood was collected within 15 minutes of taking TcB-C & TcB-UC and blood was sent to the laboratory immediately without exposing it to light. Sample size: Calculation is based on a two-sided alpha of 0.05 and a power of 90% and using a standard deviation of 2.5 mg/dl. To determine a difference in the means of 2 mg/dl, we required 70 infants. We used student’s t-test to compare the TcB_C, TcB_UC with TSB. Statistical Analysis: We used repeated measures ANOVA (analysis of variance) and student’s t-test to compare the TcB with serum bilirubin. A P value of <0.05 was chosen for statistical significance. Transcutaneous Bilirubinometry in Preterm Infants During and After Phototherapy Sadia Ansari MD*, Mike Malloy MD & Sunil Jain MD# University of Texas Medical Branch, Galveston * 3rd Year resident, # mentor Introduction Results We included 71 infants in the study (Table 1) with mean gestational age (33.4+1.4 weeks) with birth weight (2.022+481 grams), male & females were equally distributed, predominant hispanic infants (62%) with 17% DAT positive (Table 1). Mean age of starting PHT is 31 hours (Figure 1) at mean bilirubin (mean of TSB, TcB_C and TcB_UC) is 8.2 + 2.6 mg/dl. Bilirubin start decreasing after 24 hours PHT exposure and after discontinuing PHT mean bilirubin rebounds (Figure 2). At start of PHT (0 hours) TSB and TcB_C is not different but TSB & TcB_UC are significantly different. After 24 hours PHT – TcB_C is higher than TSB but after 48, 65 & 89 hours after PHT TcB_C & TSB are not statistically different than TSB. At the same time TcB_UC is significantly lower than TSB at 46, 65 & 89 hours after PHT exposure. TcB_UC remains significantly lower than TcB_C after 46, 65 & 89 hours of PHT exposure. Finally, 24 hour after discontinuing PHT, TcB_C remains significantly higher than TSB and TcB_UC (Figure 3). Background: Neonatal hyperbilirubinemia (NH) occurs in > 2/3rd term & late preterm infants (LPI) (1). Estimation of serum bilirubin (TSB) by visual inspection of the skin is not accurate(1). Transcutaneous measurement (TcB) is noninvasive, fast, convenient, inexpensive & reliable method (2) in infants from different ethnic backgrounds (3). Academy of Clinical Biochemistry laboratory medicine practice guidelines concluded that the TcB measured by BiliChek is comparable to TSB (3) by using multiple wavelengths (400 to 760 nm) which allows correction for skin pigmentation and hemoglobin concentration. Measurement of TSB requires painful heel sticks (5). NH is treated with phototherapy (PHT) which blanches skin & affects TcB . However, the blanching effect of PHT occurs only on the PHT exposed skin (12). Objective: This prospective cohort study is designed to evaluate the accuracy of TcB measurement from covered (TcB-C) skin during & after discontinuing PHT in preterm (30 – 366 weeks) infants. Description of intervention/study Summary • In preterm infants (30 – 36 weeks gestational age) receiving PHT for the treatment of NH – • At strat of PHT TcB_C, TcB_UC & TSB are not significantly different. • TcB_C correlates with TSB after 46, 65 and 89 hours of PHT exposure • TcB_UC remains significantly lower than TSB and TcB_C after 48, 65& 89 hours of PHT exposure. • 24 hours after discontinuing PHT – TcB_C is significantly higher than TSB and TcB_UC • Conclusions • In preterm infants • TcB_C is a reliable method of bilirubin estimation after 24 hours of PHT exposure • TcB_C remains reliable bilirubin measurement after 46, 65 & 89 hours of PHT exposure • 24 hours after discontinuing PHT, TcB_C is not a reliable method of bilirubin estimation. • It takes longer than 24 hours for TcB_C to equilibrate with TSB. • Future Study • In premature infants (30 – 36 weeks gestational age) - • Follow TcB_C longer than 24 hours (72 hours). • Follow TcB_C with TSB every hours to find out time of equilibrium between TSB & TcB_C References 1. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. Pediatrics 2004;114:297–316. 2. Slusher TM, Angyo IA, Bode-Thomas F, Akor F, Pam SD, Adetunji AA, et al. Transcutaneous bilirubin measurements and serum total bilirubin levels in indigenous African infants. Pediatrics 2004;113:1636–41. 3. Nichols JH, Christenson RH, Clarke W, Gronowski A, Hammett-Stabler CA, Jacobs E, et al. Executive summary. The National Academy of Clinical Biochemistry Laboratory Medicine Practice Guideline: evidence-based practice for point-of-care testing. Clin Chim Acta 2007;379:14–28. 4. Madsen LP, Rasmussen MK, Bjerregaard LL, Nøhr SB, Ebbesen F. Impact of blood sampling in very preterm infants. Scand J Clin Lab Invest 2000;60:125–32. 5. Jangaard KA, Curtis H, Goldbloom RB. Estimation of bilirubin using BiliChek, a transcutaneous bilirubin measurement device: effect of gestational age and use of phototherapy. Paediatr Child Health 2006;11:79–83. 2012 Texas Pediatric Society Electronic Poster Contest Insert Program or Hospital Logo

![[Insert Hospital Name]](https://cdn0.slideserve.com/59021/insert-hospital-name-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/1968686/slide1-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/2208608/slide1-dt.jpg)