Download
1 / 24
330 likes | 1.32k Views
Croup and Bronchiolitis. Karen D. Sawitz, MD St. Barnabas Hospital Department of Pediatrics. The Pediatric Airway. Croup - Epidemiology. 15% of respiratory visits in children Most common cause of stridor in children Primarily 1 to 6 years, mean 18 months Boys > girls (1.5 to 1)

E N D
Croup and Bronchiolitis Karen D. Sawitz, MD St. Barnabas Hospital Department of Pediatrics
Croup - Epidemiology • 15% of respiratory visits in children • Most common cause of stridor in children • Primarily 1 to 6 years, mean 18 months • Boys > girls (1.5 to 1) • Peak incidence in US 5 per 100 in 2nd yr • Predominates during fall and winter
Croup - Etiology • Viral-mediated inflammatory condition • AKA laryngotracheitis, laryngotracheobronchitis • Affects vocal cords and subglottic airway • 65% due to parainfluenza types 1, 2, 3 • Most hospitalized cases are type 1 • Others: adenovirus, RSV, varicella, measles, HSV, enteroviruses, Mycoplasma pneumoniae, and influenza A and B • Transmitted by inhalation via nasopharynx
Croup – Clinical Presentation • Prodrome: rhinorrhea, pharyngitis, low-grade fever, +/- cough over 12-48 hours • Gradual development of barking cough, hoarseness, varying inspiratory stridor +/- fever • May develop more severe obstruction with inspiratory stridor at rest, increased HR/RR, nasal flaring, retractions, progressive hypoxia and cyanosis • Symptoms may worsen at night/with crying • Mild course 3-7 days, more severe 7-14 days
Inspiratory Stridor None (0 points) When agitated (1 points) On/off at rest (2 points) Continuous at rest (3 points) Retractions None (0 points) Mild (1 points) Moderate (2 points) Severe (3 points) Air Movement/Entry Normal (0 points) Decreased (1 points) Moderately decreased (2 points) Severely decreased (3 points) Cyanosis (Color) None (0 points) Dusky (1 point) Cyanotic on room air (2 points) Cyanotic with supplemental oxygen (3 points) Level of Alertness (Mentation) Alert (0 points) Restless or anxious (1 points) Lethargic/Obtunded (2 points) <4 Mild 5-6 Mild-Moderate 7-8 Moderate 9-10 Severe Westley Croup Score
Croup – Differential Diagnosis • Infectious • Acute epiglottitis • Bacterial Tracheitis • Retropharyngeal or peritonsillar abscess • Noninfectious • Angioneurotic edema • Foreign body aspiration
Croup - Treatment • Home Management • Cool mist or night air • Steam (vaporizer or from shower) • Keep child calm • Primary Care/ER Setting • Cool mist (may precipitate bronchospasm) • Steroids: oral or IM dexamethasone 0.6 mg/kg single dose (half-life 36-52 hours) • Racemic epinephrine in severe cases: 0.25-0.5 ml in 2.5 ml saline by nebulizer
Croup - Treatment • Criteria for discharge after Racemic Epi • Observation for 3-4 hours • No stridor at rest • Normal air entry • Normal color • Normal level of consciousness • Have received a dose of dexamethasone
Croup – Indications for Admission • Suspected or actual epiglottitis • Cyanosis/hypoxemia/pallor • Stridor at rest or progressive stridor • Respiratory distress • Depressed sensorium • Restlessness • Toxic appearance Nelson Textbook of Pediatrics 16th Edition 2000
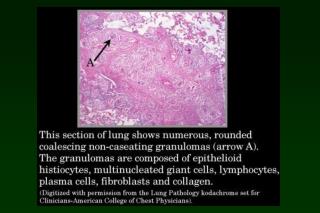
Bronchiolitis - Epidemiology • Most common lower respiratory tract infection in infants • Most common etiology is RSV, most cases between December and March (75% of cases under 2) • More common in crowded living conditions and smoke exposure • Breastfeeding appears to confer a protective advantage • Most severe symptoms in those under 2 • >50% affected by age 1, 80-90% by age 2, 40% have LRTI • No permanent RSV immunity, reinfections common • 1-2% require hospitalization • 90,000 hospitalizations annually (80% under 1 year) • Deaths 4500 (1985) 510 (1997) 390 (1999) • Cost of hospitalization infants under 1 year: $700 mil/yr • More likely to have respiratory problems when older
RSV Spread • Humans only source of infection • Direct or close contact with secretions • Large-particle droplets <3 ft or fomites • May persist hours on surfaces or 30 minutes on hands • Viral shedding 3-8 days or longer • Incubation period 2-8 days (4-6)
Bronchiolitis – Clinical Features • Pathophysiology • Marked inflammation, edema, necrosis of smaller airway epithelial cells • Increased mucus production • Bronchospasm • Clinical Features • Rhinitis, tachypnea, wheezing, cough, crackles • Accessory muscle use and nasal flaring • Apnea, grunting, cyanosis • Poor feeding, difficulty sleeping, fussiness • Tachycardia and dehydration may occur • Natural course 7-10 days, peak on day 4
Bronchiolitis – Diagnosis & Testing • Clinical diagnosis on basis of H & P • Laboratory and radiologic studies should not routinely be ordered per AAP • NP swab for RSV ELISA may be used eg for cohorting • CXR to exclude other Dx, or if not improving as expected • Concurrent SBI is rare, may need to be ruled out in febrile young infants (UTI)
Bronchiolitis – Risk Factors for Severe Disease • Age under 6-12 weeks • History of prematurity esp < 28 weeks GA • Underlying cardiopulmonary disease • Chronic lung disease (BPD, CF) • Complex congenital heart disease • Congenital airway abnormalities • Immunodeficiency • Severe neuromuscular disease
Bronchiolitis - Management • Mainstay: supportive care (hydration, oxygenation, nasal suction, respiratory support if needed) • No routine bronchodilator use – may improve symptoms short-term but no effect on length of illness or LOS; potential for harm (SE, cost) • No routine corticosteroid use – no benefit in RR, O2 sat, LOS though given to 60% of inpatients • No routine use of ribavirin – variable results, may be appropriate for severely ill infants • Antibiotics only if indication of concurrent bacterial infection
Bronchiolitis – Criteria for Admission • Persistent hypoxia • Respiratory distress • Inability to tolerate fluids • Inability to ensure close follow-up • Infants under 2 months of age - consider • Premature infants - consider
RSV Bronchiolitis - Prevention • Palivizumab (Synagis®) prophylaxis for selected infants under 24 months • 15 mg/kg IM monthly November-March • Hand washing • Avoiding passive smoke exposure • Promotion of breastfeeding
Criteria for Passive Immunization • ≤24 mos old with • CLD on therapy in 6 mos before start of RSV season • Hemodynamically significant congenital heart disease • ≤32 weeks GA even without CLD • <28 wks GA during first season/≤12 mos at start • 29-32 wks GA up to 6 mos of age at start of season • 32-35 wks GA up to 3 mos with ≥1 risk factor: • Day care attendance or • Sibling under 5 years of age • <34 wks GA with airway abn or neuromuscular dz Source: AAP Red Book 2009