Download
1 / 1
10 likes | 86 Views
An Exploratory Analysis of Functioning Across Biosystemic Levels of Organization in Inpatients and Outpatients with Serious Mental Illness

E N D
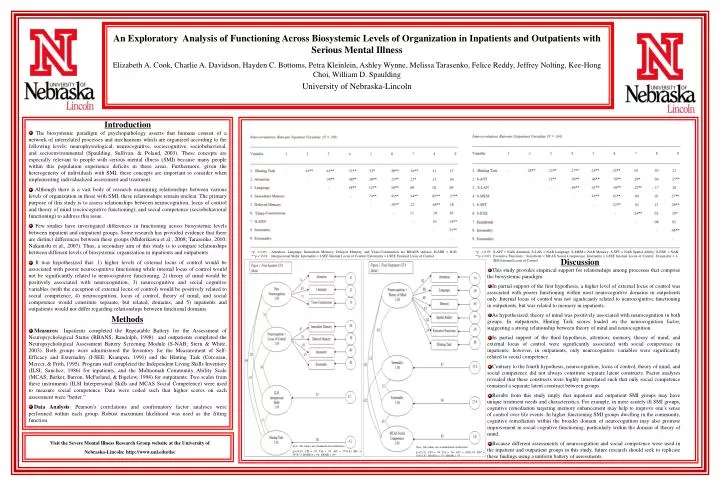
An Exploratory Analysis of Functioning Across Biosystemic Levels of Organization in Inpatients and Outpatients with Serious Mental Illness Elizabeth A. Cook, Charlie A. Davidson, Hayden C. Bottoms, Petra Kleinlein, Ashley Wynne, Melissa Tarasenko, Felice Reddy, Jeffrey Nolting, Kee-Hong Choi, William D. Spaulding University of Nebraska-Lincoln Introduction • The biosystemic paradigm of psychopathology asserts that humans consist of a network of interrelated processes and mechanisms which are organized according to the following levels: neurophysiological, neurocognitive, sociocognitive, sociobehavioral, and socioenvironmental (Spaulding, Sullivan, & Poland, 2003). These concepts are especially relevant to people with serious mental illness (SMI) because many people within this population experience deficits in these areas. Furthermore, given the heterogeneity of individuals with SMI, these concepts are important to consider when implementing individualized assessment and treatment. • Although there is a vast body of research examining relationships between various levels of organization in those with SMI, these relationships remain unclear. The primary purpose of this study is to assess relationships between neurocognition, locus of control and theory of mind (sociocognitive functioning), and social competence (sociobehavioral functioning) to address this issue. • Few studies have investigated differences in functioning across biosystemic levels between inpatient and outpatient groups. Some research has provided evidence that there are distinct differences between these groups (Midorikawa et al., 2008; Tarasenko, 2010; Nakanishi et al., 2007). Thus, a secondary aim of this study is to compare relationships between different levels of biosystemic organization in inpatients and outpatients. • It was hypothesized that: 1) higher levels of external locus of control would be associated with poorer neurocognitive functioning while internal locus of control would not be significantly related to neurocognitive functioning, 2) theory of mind would be positively associated with neurocognition, 3) neurocognitive and social cognitive variables (with the exception of external locus of control) would be positively related to social competence, 4) neurocognition, locus of control, theory of mind, and social competence would constitute separate, but related, domains, and 5) inpatients and outpatients would not differ regarding relationships between functional domains. *p < 0.05 **p < 0.01 Attention, Language, Immediate Memory, Delayed Memory, and Visuo-Construction are RBANS indexes; ILSIIN = ILSI Interpersonal Skills; Internality = I-SEE Internal Locus of Control; Externality = I-SEE External Locus of Control *p < 0.05 **p < 0.01 S-ATT = NAB Attention; S-LAN = NAB Language; S-MEM = NAB Memory; S-SPT = NAB Spatial Ability; S-EXE = NAB Executive Functions; Socialtotal = MCAS Social Competence; Internality = I-SEE Internal Locus of Control; Externality = I-SEE External Locus of Control Discussion • This study provides empirical support for relationships among processes that comprise the biosystemic paradigm. • In partial support of the first hypothesis, a higher level of external locus of control was associated with poorer functioning within most neurocognitive domains in outpatients only. Internal locus of control was not significantly related to neurocognitive functioning in outpatients, but was related to memory in inpatients. • As hypothesized, theory of mind was positively associated with neurocognition in both groups. In outpatients, Hinting Task scores loaded on the neurocognition factor, suggesting a strong relationship between theory of mind and neurocognition. • In partial support of the third hypothesis, attention, memory, theory of mind, and external locus of control were significantly associated with social competence in inpatients; however, in outpatients, only neurocognitive variables were significantly related to social competence. • Contrary to the fourth hypothesis, neurocognition, locus of control, theory of mind, and social competence did not always constitute separate latent constructs. Factor analyses revealed that these constructs were highly interrelated such that only social competence remained a separate latent construct between groups. • Results from this study imply that inpatient and outpatient SMI groups may have unique treatment needs and characteristics. For example, in more acutely ill SMI groups, cognitive remediation targeting memory enhancement may help to improve one’s sense of control over life events. In higher functioning SMI groups dwelling in the community, cognitive remediation within the broader domain of neurocognition may also promote improvement in social cognitive functioning, particularly within the domain of theory of mind. • Because different assessments of neurocognition and social competence were used in the inpatient and outpatient groups in this study, future research should seek to replicate these findings using a uniform battery of assessments. Methods • Measures:: Inpatients completed the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS; Randolph, 1998) and outpatients completed the Neuropsychological Assessment Battery Screening Module (S-NAB; Stern & White, 2003). Both groups were administered the Inventory for the Measurement of Self-Efficacy and Externality (I-SEE; Krampen, 1991) and the Hinting Task (Corcoran, Mercer, & Frith, 1995). Program staff completed the Independent Living Skills Inventory (ILSI; Sanchez, 1986) for inpatients, and the Multnomah Community Ability Scale (MCAS; Barker, Barron, McFarland, & Bigelow, 1994) for outpatients. Two scales from these instruments (ILSI Interpersonal Skills and MCAS Social Competence) were used to measure social competence. Data were coded such that higher scores on each assessment were “better.” • Data Analysis: Pearson’s correlations and confirmatory factor analyses were performed within each group. Robust maximum likelihood was used as the fitting function. Visit the Severe Mental Illness Research Group website at the University of Nebraska-Lincoln: http://www.unl.edu/dsc Note. All values are standardized coefficients. χ2=30.93, CFI = .95, TLI = .95, AIC = 5776.63, BIC = 5878.72, RMSEA = .04, SRMR = .09 Note. All values are standardized coefficients. χ2=32.51, CFI = .98, TLI = .96, AIC = 10421.87, BIC = 10514.87, RMSEA = .05, SRMR = .05






